- Weight loss with hypothyroidism requires fixing the root cause with proper thyroid medication, not just diet and exercise alone, since hormone imbalance prevents fat loss.
- Get complete thyroid testing including free T3, free T4, and reverse T3 to identify conversion problems that standard TSH tests miss.
- Add T3 thyroid hormone in doses of 10-25 mcg daily alongside your T4 for significantly better weight loss results than T4-only therapy.
- Combine thyroid medication optimization with high protein intake (100+ grams daily), adequate carbs, and consistent exercise for sustainable fat loss.
Did you know that losing weight with hypothyroidism doesn’t have to be impossible?
As a specialist in helping patients with Hypothyroidism and Hashimoto’s, I’ve been able to personally help hundreds of patients lose weight. And today I want to share with you how I do it.
I’m going to teach you how to lose weight with hypothyroidism by giving you the recommendations that I give to my patients.
I will also go over case studies of real-life patients that I’ve been able to help and provide you with what tests you need to get from your doctor to get to the root cause of your weight loss resistance.
So let’s jump in…
Why Weight Loss is so Difficult with Hypothyroidism
Does this scenario sound familiar…
You’ve been restricting your calories to try to lose weight, but every time you do, you get more fatigued than normal.
You’ve been able to lose 5-10 pounds by doing this, but once you start eating normally again, your weight pops RIGHT back up to where it was.
This is something that I’ve seen over and over again, and it’s something that we need to discuss.
Calorie-restricted diets are not the best way to lose weight, and they can actually be harmful to those with hypothyroidism.
And this really shouldn’t come as a surprise.
After all, how many times have you tried these types of diets? How many times have they worked for you? And, did they actually help you lose weight and keep it off?
You know that they don’t work, even without looking at the numbers, but in case you were wondering, you have about a 1 in 200 chance of losing weight and keeping it off by using this type of diet.

But why is this? Why is it so hard to lose weight? Why do some people say it’s impossible?
Much of this may have to do with the way that we look at weight loss, what causes weight gain, and how we approach treatment.
For instance:
We know that restricting calories results in changes to your thyroid function which may result in a reduction in your metabolic rate (1).
This effect is mediated through the changes that your body goes through during starvation and how those changes impact your hypothalamus and TRH (parts of the thyroid axis).
If you’re trying to lose weight, do you really want to lower your metabolism in the process?
Of course not, but it appears that thyroid function may be a casualty in the dieting process.
By limiting your calories, you’re actually telling your body that you don’t have enough calories to survive, so your body starts to lower your metabolism to protect itself.
It lowers your metabolism by reducing the active amount of Thyroid hormone or Free T3 Levels (2).
It also does this by increasing reverse T3 levels (3)!
Oddly enough, all of these changes are also seen in a condition known as euthyroid sick syndrome which occurs when people are critically ill.
It’s certainly possible that dieting creates a metabolic process that mimics the same process that occurs when you are sick or fighting off an infection.
And the problems don’t stop there:
Most physicians, while well-meaning, tend to prescribe the ‘eat less, exercise more’ mantra, which may potentially make the problem worse.
So if losing weight isn’t about restricting calories, then how do you do it?
- Bottom Line: Do NOT restrict your calories if you have Hypothyroidism for weight loss. It will only make your thyroid function worse in the long term.
Losing Weight is About Balancing Your Hormones
While calorie restriction may be an important part of losing weight, you have to look beyond the calories and into your hormones.
If losing weight were as simple as burning more calories than you consume, we wouldn’t see graphs like this:
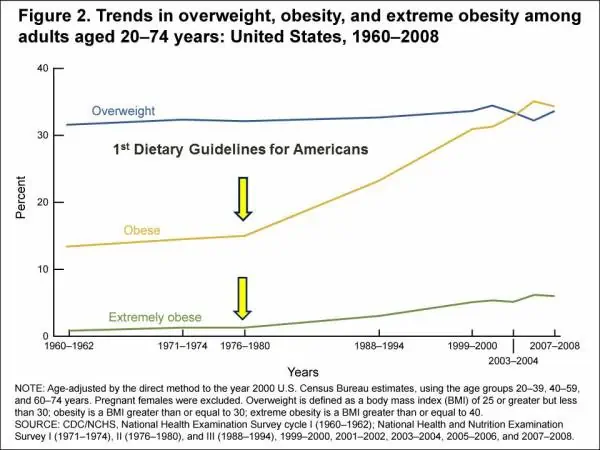
Because we know that people have been exercising more than ever and cutting back on the number of calories that they consume, and they’ve been doing this for 30+ years.
So, back to the hormones for a minute.
Your hormones are incredibly powerful, and they play an important role in how your body processes calories.
You can think of your hormones as gatekeepers that direct calories to the tissues that need them.
For instance:
Under the influence of insulin, your body may direct calories to your fat cells for storage as opposed to your skeletal muscles (4).
In this setting, you wouldn’t want to have increased insulin because that would result in fat cell growth.
Under the influence of testosterone, on the other hand, your skeletal muscles take up calories and energy to burn it and produce muscle growth (5).
Would you rather have your fat cells take that energy or your muscle cells?
The answer is obvious, but what you don’t realize is that the distinction between these two events is not the number of calories that you consume but the absolute level of each hormone.
When you understand this simple idea, it’s easy to understand how you can gain fat mass despite eating a “normal” amount of calories.
Losing weight and keeping it off is, therefore, about optimizing the relative concentrations of these hormones to help put your body in a state in which it can burn calories without storing them.
And, this process is well-studied and not very difficult to follow.
The problem is that the vast majority of physicians are not trained in how to manage hormone imbalances; it’s just not what they were trained to do.
But that doesn’t make this information any less valid as there’s plenty of research to confirm how these hormones influence fat mass, muscle mass, and weight gain.
Let me go over some examples of how this works to help you understand what I’m talking about here.
Real Patient Case Studies & How They Lost Weight
These are all real-life patients from my former practice. Once you have the right understanding of why people can’t lose weight, and you know what to test for, it becomes easy to treat patients with weight loss resistance.
Before we get into the most common hormonal imbalances, we need to start with the basics.
If you want to lose weight you will have to optimize your thyroid function FIRST.
None of the other hormonal systems will come into balance if your thyroid function looks like this…
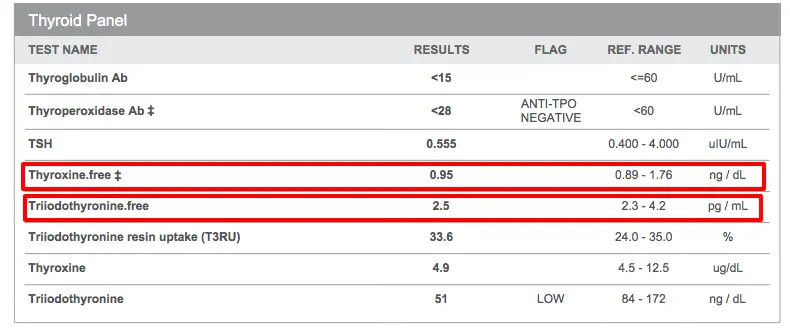
This is technically a “normal” test, but this patient had ALL of the symptoms of hypothyroidism, and yes was told her labs were “normal”.
Once she was given thyroid hormone (Armour thyroid in this case), she lost weight and had an almost complete resolution of her symptoms.
This concept holds true for patients who are being under-treated or are being treated with the wrong type of medication, too!
Before you check other hormones, start with your Thyroid function.
You can find 4 simple tests to see if your thyroid function is up to par here.
I’ve found that most patients do better on some form of T3 in their thyroid hormone.
That means Natural Desiccated Thyroid or some form of liothyronine, either by itself or with Levothyroxine.
Once you feel your thyroid function is optimized, then you can jump into evaluating and testing for other hormonal imbalances.
#1. Insulin Resistance, Elevated Blood Sugar, and Pre-Diabetes
We are discussing insulin resistance first because it’s incredibly common, and many patients aren’t aware that they suffer from it.
From a purely statistical standpoint, you have about a 1 in 2-3 chance (or 50%) of having pre-diabetes or diabetes as an adult in the US.
The CDC estimates that around 84.1 million people in the United States have pre-diabetes and around 30.3 million people have diabetes.
Insulin resistance is the condition that leads to diabetes, pre-diabetes, high blood sugar, heart disease, Alzheimer’s, and so on.
The reason that this condition can go unnoticed is that, initially, insulin levels tend to rise before blood sugar rises.
So, if you are only looking at blood sugar, then you may miss the early diagnosis of insulin resistance.
One of the best ways to identify insulin resistance early is by evaluating serum fasting insulin levels (in addition to blood glucose).


In this example, you can see that this patient has pre-diabetes based on her Hgb A1c, but she also has an extremely high fasting insulin of 22.1 uIU/mL.
The best “range” for weight loss, when it comes to insulin, is as low as possible, but ideally less than 5 uIU/mL.
Excessively high levels of insulin will block your body from burning fat as an energy source, and it does this by manipulating an enzyme known as hormone-sensitive lipase (6).
The net result will be an increased appetite and the need for frequent snacking in order to maintain blood glucose.
As you can see from the image above, in order to burn fat as an energy source, insulin levels must be low.
In this patient, we were able to help drive down your insulin levels by focusing on a number of treatments, including:
- Intermittent fasting regimen (7) (variation of calorie restriction)
- Medications designed to lower insulin resistance
- Supplements designed to lower blood sugar and insulin resistance
- Exercise routine (8) (strength training and interval training)
- Changes to her diet
These strategies work incredibly well for many patients and even work for those suffering from diabetes (9).
Quick tips to remember if you are suffering from insulin resistance:
- Lab Tests: Check fasting insulin levels (this should be < 5), Hgb A1c (should be less < 5.3), and fasting glucose levels (should be < 85). If you are doing a fasting protocol, make sure to check your fasting insulin level at the end of your fast to ensure that your level is < 5. Do NOT attempt fasting if you are on insulin, as it may cause harm due to hypoglycemia.
- Treatment: Find a Functional Medicine doctor who will work with you on the following: LCHF diet (if appropriate for your thyroid function and adrenal function), intermittent or prolonged fasting programs, and high-intensity interval training. If you are looking for supplements, I recommend the following: Berberine and Curcumin. Berberine has been shown in studies to be as effective as Metformin in lowering Hgb A1c (10), and Curcumin has been shown to prevent the onset of diabetes from pre-diabetes for 9 months (11).
#2. Thyroid Resistance and Leptin Resistance
Thyroid resistance and leptin resistance are both seen in patients who have undergone metabolic damage from repeated yo-yo dieting.
Yo-yo dieting refers to a state in which your body weight is constantly fluctuating.
Each time you undergo a new fad diet, you are able to lose some weight, but that weight returns after you stop the diet.

This process continues on and on over the years, and the constant fluctuation causes a series of hormone changes that can be measured and tracked in your body.
Repeated weight loss and weight gain result in leptin resistance.
Your fat cells are supposed to tell your brain when they are “full”, which is supposed to trigger your brain to increase metabolism to burn up the extra fat.
The repeated weight loss/weight gain cycle disturbs this communication and results in a condition where your brain becomes less sensitive to the hormone leptin.
Your fat cells produce leptin, but your brain is resistant to the message.
So your brain thinks that leptin levels are low when, in reality, they are very high.
This results in a reduction in your metabolism and an increase in your appetite (13), which are the hallmark symptoms of leptin resistance.
Leptin also appears to have an impact on your thyroid function and vice versa.
We know that your thyroid helps to control your metabolism, and we also know that leptin plays a role in regulating both metabolism and thyroid hormone.
In addition, studies have shown that calorie-restricted diets tend to cause changes to your thyroid function, which limit the active thyroid hormone T3 (14).
It could be that dieting and repeated weight gain and weight loss cause the following chain reaction:
- Dieting causes low free T3 and high reverse T3
- These changes in thyroid hormone trigger the release of leptin to try to improve metabolism
- The brain becomes resistant to increasing leptin levels, and you become leptin-resistant
- The more you continue to diet to lose weight, the more damage to your thyroid you incur, which worsens leptin resistance
Your lab results, if you suffer from this condition, may look something like this:
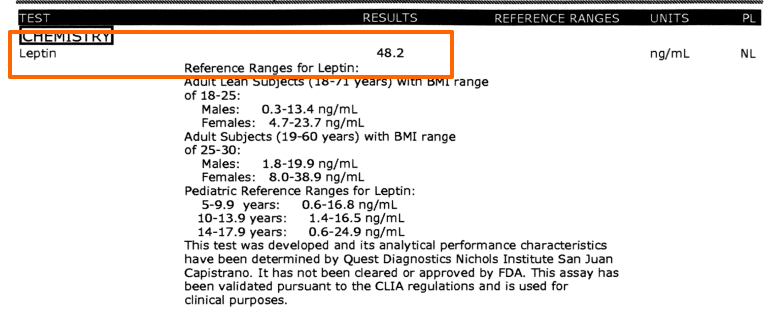
An elevated fasting leptin, in the presence of obesity, is a sign that you may be suffering from leptin resistance.
You’ll probably also find that if you order a complete thyroid lab panel, your free T3 and total T3 are probably also low.
The lab results you see above are from a patient who had a history of repeated HCG dieting.
These diets are notorious for causing damage to your metabolism and may ultimately lead to leptin resistance.
In these situations, treatment must focus on both thyroid dysfunction and leptin dysfunction.
T3-containing medications are particularly effective at improving free T3 and total T3 levels, while other medications, such as GLP-1 agonists, can help treat leptin resistance.
Think you have Leptin resistance or thyroid Resistance?
Here’s what you need to do:
- Lab Tests: Check fasting serum Leptin levels (< 12 is considered normal), anything > 12 is considered Leptin resistance. Check your Free T3/Reverse T3 ratio. This will tell you if you have too much thyroid-blocking hormone relative to free and active Free T3. Your ratio should be > 0.2 (anything less is thyroid resistance).
- Treatment: Thyroid resistance responds best to NDT and/or Liothyronine or sustained-release T3. You should monitor Reverse T3 levels regularly while on T3 to find out when you “wash” out the reverse T3 levels. Once they go down to < 5, you can back down on Free T3 levels. About 2/3 of patients respond to NDT, and about 1/3 will need Pure T3.
#3. Estrogen Dominance & Low Progesterone
Estrogen and progesterone are both considered to be sex hormones and are very important for female growth and development.
Think about it:
Estrogen helps to develop breast tissue, and ovarian tissue (15), helps regulate your menstrual cycle (16), and the decline in estrogen is what triggers menopause (17).
Excessively high estrogen is a condition that results in PCOS, menstrual irregularity, PMS/PMDD, endometriosis, and so on.
This condition is often referred to as ‘estrogen dominance’, which simply means that you have an excessively high level of estrogen in your body.
The main problem with excess estrogen is that it can lead to weight gain and fat cell growth.
This growth is usually concentrated in specific areas of the body, including the hips, butt/gluteal region, and thigh region.
This fat cell growth is a good thing when it’s under control. After all, it is the growth of these areas that gives women their curves and the characteristic female phenotype.
But, when the growth is excessive, then it becomes a problem.
Estrogen dominance is also becoming more and more common.
Obesity, lack of exercise, insulin resistance, declining progesterone, and hypothyroidism can all lead to excess estrogen.
Estrogen dominance tends to occur in 3 different ways (and each is important for understanding how to treat it):
1. Too much estrogen with “normal” progesterone levels.
2. Too little progesterone with “normal” estrogen levels.
3. Excessive exposure to xenoestrogens from the environment with “normal” estrogen and progesterone levels.
Usually, most women know if they have an estrogen/progesterone imbalance simply based on their symptoms alone.
High levels of estrogen tend to cause very specific symptoms that are hard to miss.
Testing for both estrogen and progesterone can be done through routine bloodwork.
However, when testing for estrogen and progesterone, it’s important to remember that these levels are constantly in flux due to the menstrual cycle.
The best time of the month to test for these hormones is during the mid-luteal phase or between days 19-21 of the menstrual cycle.
You should then look at the relative difference between both estrogen and progesterone to determine if your values are “normal”.
It’s helpful to have an idea or a baseline set of labs to compare your results with, considering that each woman will have a different definition of “normal”.
More advanced testing also exists:
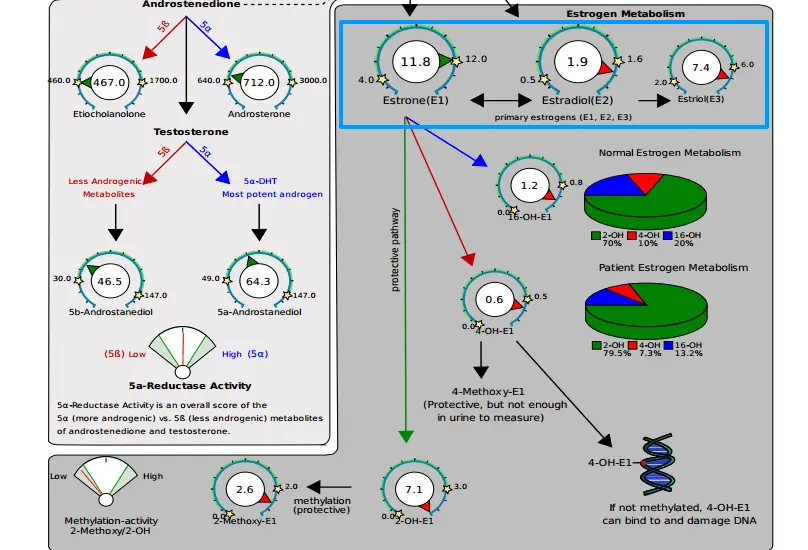
Urinary levels of both estrogen and estrogen metabolites (estradiol, estriol, and estrone) can help you understand how your body is processing and metabolizing estrogen.
In this example above, you can see that estrogen is being blocked at the last stage of elimination.
Once we optimized her liver function, put her on herbs to help eliminate estrogen down the protective 2-hydroxy pathway (18), and opened up her ability to methylate with activated B vitamins, she was able to lose weight and eliminate excess estrogen.
If you think you are suffering from estrogen dominance, you can do the following:
- Lab Tests: Check serum estradiol and progesterone at the same time on days 19-22 of your menstrual cycle. You can also order more advanced tests via urinary estrone, estradiol, and estriol plus metabolites (16-hydroxy Estrone, 4-hydroxy Estrone, and 2-hydroxy Estrone) on day 19-22 of the mid-luteal phase of your menstrual cycle.
- Treatment: Clean up and improve liver function, increase consumption of cruciferous vegetables (19), consider FAR infrared sauna use, and consider supplementing with DIM or Indole-3-Carbinol to help metabolize excess estrogen through the liver. Depending on progesterone levels you may also benefit from using Bio-identical Progesterone cream.
#4. Low Testosterone with Insulin Resistance
We often tend to think of testosterone as a male sex hormone, but it’s very important for women too.
In women (and men), testosterone helps build lean muscle mass, helps promote fat loss, helps control your libido (20), and helps regulate your mood.
Women with low testosterone may feel “flabby”, find it difficult to gain muscle mass, find it difficult to lose weight, and may experience mood problems like irritability or depression.
Low testosterone can even contribute to a low sex drive or decreased libido!
Testosterone can be easily tested in the serum by ordering free and total testosterone:

Low testosterone is very common among women as they age (much like men) and in certain medical conditions, including hypothyroidism.
This patient has low-normal testosterone lab tests but was experiencing symptoms, including decreased libido and weight gain.
Upon replacement, these symptoms subsided rapidly.
In addition, testosterone (especially in women) can be impacted by other hormones such as insulin.
Insulin resistance and high blood sugar can negatively impact testosterone and lead to low testosterone or high testosterone (21) (depending on the woman):
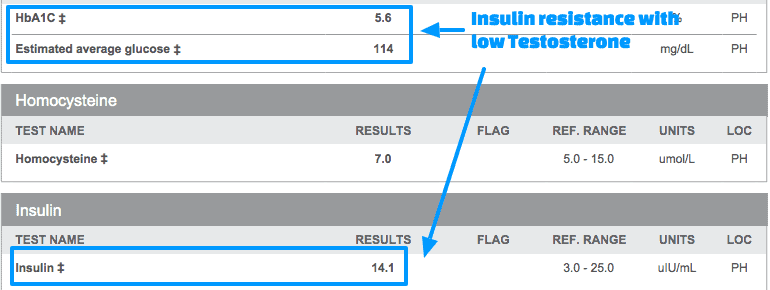
This particular patient was suffering from both Low testosterone and insulin resistance.
Insulin resistance and testosterone dysregulation are often seen together, and it’s very important to treat both if weight loss is your goal.
In this patient, once we gave her some bioidentical low-dose testosterone, she was able to lose weight, build muscle, and improve her mood.
In addition, it was easier to reverse her insulin resistance as opposed to using dietary measures alone.
If you think low testosterone and/or insulin resistance is contributing to your weight loss resistance, consider these steps:
- Lab Tests: Check free and total Testosterone. Optimal levels depend on the patient and their symptoms; however, in general, I like to see testosterone in the mid-range for women unless they have a history of autoimmune disease or Hashimoto’s. Patients with autoimmune disease tend to have both low DHEA (22) and testosterone levels and may do better with high-normal levels.
- Treatment: If Testosterone levels are low I would consider using bio-identical testosterone cream. Start low dose and check testosterone levels after 4-8 weeks. Also, check for insulin resistance and treat aggressively if present, treating insulin resistance may cause a natural increase in Testosterone levels.
#5. Adrenal Fatigue with Elevated Cortisol
Adrenal fatigue is another extremely common hormonal imbalance in patients with hypothyroidism.
Cortisol is a hormone that your body calls upon in times of stress and why it is considered to be the ‘stress hormone’.
One of the main issues with cortisol is that it appears to be connected or linked to thyroid hormones in some way.
As thyroid hormone changes it impacts cortisol.
In hypothyroid states, it’s possible for cortisol to become dysregulated either in absolute value or at the receptor level.
In either event, the end result may be decreased weight loss or weight loss resistance.
Excessively high levels of cortisol also contribute to hormone imbalances such as insulin resistance.
And long-term exposure to cortisol has been shown to contribute directly to weight gain, especially in the belly area (23).
Patients with cortisol dysregulation often experience the following symptoms:
- Extreme fatigue
- Weight loss resistance
- Weight gain especially in the belly
- Food cravings for sugar and salt
- Feeling “wired but tired”
- Anxious or jittery feeling
You can test for cortisol with a simple serum blood test but there are also many other ways to assess for cortisol including urinary and salivary levels.
Always start first with an 8 am serum cortisol level and then work your way into other tests as necessary.
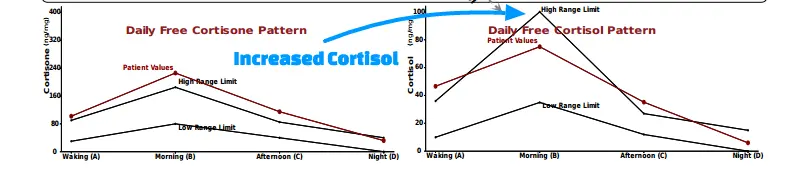
The image above represents a series of 4 cortisol urinary tests throughout the day.
You can see that the cortisol levels spike in the early morning around the time that most people consume coffee or caffeine.
This type of pattern is common among those with high-stress jobs, those who sleep 6 or fewer hours per night, and those who are under constant stress.
This particular patient was experiencing persistent weight gain and dealing with the other symptoms of adrenal fatigue.
Treating cortisol dysregulation can be accomplished with adaptogenic herbs and supplements, by reducing your exposure to stress and by cutting back on caffeine.
If you suspect that you have abnormal cortisol levels then consider these steps:
- Lab Tests: Start with serum cortisol. From there you can determine if salivary or urinary cortisol is necessary.
- Treatment: If Cortisol levels are elevated consider a combination of the following: removing caffeine and stimulants, adding higher doses of salt into your diet, eating smaller more frequent meals, using stress reduction techniques, and supplementing with adrenal glandulars or adaptogens. All of these therapies have been shown to be effective at reducing the negative impact stress has on the body.
How to Test for these Hormonal Imbalances
If after reading the above section you think you have a hormonal imbalance simply go down to the area and look at the tests.
It will show you which tests you need to order to evaluate your hormones and show you the reference levels your results should fall into.
Remember that there is a big difference between being “normal” and being “optimal”.
Don’t let someone tell you that your labs are “normal” if you feel like crap. It’s not that your labs are normal, it’s that the doctor isn’t ordering the right tests or he/she isn’t interpreting them correctly.
Testing For Hormonal Imbalances
| Test | Optimal Levels for Health | |
| Thyroid Deficiency | Blood: · TSH, Free T3, Free T4, Reverse T3, Thryoglobulin Antibodies, Thyroperoxidase Antibodies, Sex Hormone Binding Globulin (SHBG), Ferritin, TIBC, Serum Iron | TSH: < 2 Free T3: 1/3 of reference range Free T4: 1/3 of reference range Reverse T3: < 15 Thyroglobulin: <15 Thyroperoxidase: < 15 SHBG: · Male: 20-30 · Female: 70-80 Ferritin: 70-80 Serum Iron: Mid range TIBC: 35-38% |
| Estrogen Dominance | Urine: · Estrone, Estradiol, Estriol, 16-hydroxy Estrone, 4-hydroxy Estrone and 2-hydroxy Estrone | Optimal levels highly variable, must be compared to Progesterone and in the setting of symptoms. Generally 2-OH Estrone should be preferred over other pathways. |
| Progesterone Deficiency | Blood: · Progesterone Urine: · Pregnanediol | Check on day 19-22 of Menstrual cycle if menstruating. Progesterone levels should be higher than Estrogen levels during days 19-22 (see image below). |
| Insulin Resistance | Blood: Insulin (Fasting and 2 hours after meals), Hemoglobin A1c (Hgb A1c), Fasting blood sugar (FBS), Uric Acid, Fasting Triglycerides, Fasting HDL | Insulin: · Fasting: < 5 · 2 hours after meal: < 30 Hgb A1c: < 5.3 FBS: < 85 Uric Acid: < 5 Fasting trig: < 100 Fasting HDL: > 60 |
| Leptin Resistance | Blood: · Leptin levels · Thyroid studies (above) · Insulin tests (above) | Leptin: < 12 |
| Cortisol and Adrenal Fatigue | Urine: · Cortisol and Cortisone x4 Salivary: · Cortisol x4 Blood: · AM Cortisol (Not very accurate) | Range is dependent upon the person and is relative. If Cortisol levels are low = Late stage adrenal fatigue. If cortisol levels are high = Early stage adrenal fatigue. |
Conclusion
Weight loss is definitely possible if you have thyroid disease but it takes the right approach.
This approach includes the evaluation of your hormones, including those beyond your thyroid.
By evaluating, diagnosing, and treating these imbalances you will be able to not only lose weight but keep it off.
While some of this information may be new to you just remember that many of these conclusions have been drawn as the result of clinical research and real-patient experiences.
You may need to read through this one or more times to let everything sink in.
It is also helpful to grab your own set of labs and compare your lab results to the patients listed in this guide.
From there you can determine the similarities or differences between you and them which may be able to help guide your treatment.
But, remember, that you are an individual and even if your test results may look similar, it doesn’t mean that you need the same treatment.
Ensure that you get the proper work-up if you think your hormones are out of balance because you shouldn’t have to go through life feeling like you’re crazy because your labs are all “normal”.
Many patients feel vindicated when they realize they actually do have abnormalities in their lab results, they just needed someone with the right knowledge to evaluate them.
Now it’s your turn:
Are you suffering from hypothyroidism?
Is it also difficult for you to lose weight?
Has anything worked well for you?
If not, why?
Leave your questions or comments below so that we can continue the conversation and continue to help future people!
Scientific References
#1. https://www.ncbi.nlm.nih.gov/pubmed/1436373
#2. https://www.ncbi.nlm.nih.gov/pubmed/10378389
#3. https://www.ncbi.nlm.nih.gov/pubmed/3757921
#4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC380258/
#5. https://www.ncbi.nlm.nih.gov/pubmed/2917954
#6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC333098/
#7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5394735/
#8. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4625541/
#9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3168743/
#10. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2410097/
#11. http://www.ncbi.nlm.nih.gov/pubmed/22773702
#12. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4069066/
#13. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3281561/
#14. https://www.ncbi.nlm.nih.gov/pubmed/12055988
#15. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3652894/
#16. https://www.ncbi.nlm.nih.gov/books/NBK279054/
#17. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2717878/
#18. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4505810/
#19. https://www.ncbi.nlm.nih.gov/pubmed/1656396
#20. https://www.ncbi.nlm.nih.gov/pubmed/26358173
#21. https://www.ncbi.nlm.nih.gov/pubmed/18319314
#22. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2701249/
#23. http://www.ncbi.nlm.nih.gov/pubmed/11020091





