
- 'Normal' thyroid labs can mask tissue-level hypothyroidism where insufficient thyroid hormone reaches your cells despite adequate blood levels. Use the free T3 to reverse T3 ratio (should be above 0.2) to catch this pattern when standard tests appear normal.
- Optimal thyroid medication matters more than dose alone. Natural desiccated thyroid (NDT) or T3-containing medications often work better than T4-only drugs for patients with inflammation, autoimmunity, or high reverse T3 levels.
- Thyroid optimization alone causes only 5-10 pounds of weight loss; the remaining weight loss comes from treating other hormone imbalances like insulin and leptin resistance through diet, supplements, and lifestyle changes.
- Avoid 'thyroid tunnel vision' by treating the whole system. You must address inflammation, gut health, nutrient deficiencies, stress, and detoxification alongside thyroid therapy to see real weight loss results.
- Expect 5-10 pounds of steady monthly weight loss over 6-12 months when you approach treatment comprehensively. Patience and consistency matter far more than quick fixes.
Contrary to what pharmaceutical companies would have you believe, you can lose weight without Ozempic, even if you have Hashimoto’s.
Is it difficult and does it take longer if you have a thyroid problem? Sure, but it’s definitely not impossible.
The reality is that good old-fashioned treatments like the right diet, exercise, supplements, and the right thyroid medication can work miracles for thyroid patients.
Today I’m going to walk you through how Melanie was able to lose over 50 pounds over the course of about 6 months with the use of natural treatments because if she can do it, you can too.
Let’s jump in:

Hashimoto’s Weight Loss Case Study
Here’s what you need to know about her:
This patient has a family history of thyroid problems (all of which were undertreated or misdiagnosed), and ever since she was a child she had issues with weight, fatigue, and decreased energy.
At an early age, she underwent radioactive iodine ablation, but 30% of her thyroid remained functional as estimated by her doctors at that time.
As a result of the ablation and her almost normal thyroid lab values, she was placed on a low dose of levothyroxine and felt terrible for about 20 years.
Over this time period, she gained weight and never saw symptomatic improvement despite taking levothyroxine faithfully so she eventually stopped taking her thyroid medication altogether.
This was not a good idea (as we will soon discuss) because she was operating with only about 30% function from her thyroid gland.
In other words, the 30% of her remaining thyroid gland was trying to keep up with the permanently damaged 70% which led to all of these problems.
She was kicked around from doctor to doctor until she was at her highest weight of 270 pounds.
Not satisfied with this result, and like a true champion, she took matters into her own hands and was able to lose 30 pounds by changing her diet and adding in exercise despite feeling exhausted 24/7.
She was able to do this with a keto-type diet but eventually hit a plateau and was unable to lose any further weight around 250 pounds.
Even though she was able to lose some weight, she still felt symptomatic from her thyroid and her symptoms remained (remember she was not on thyroid medication during this time).
Optimal vs Normal Thyroid Lab Tests: Why she was undertreated for years
The most interesting part of her story is that she was only ever treated with a low dose of levothyroxine despite seeking care from multiple endocrinologists and primary care physicians.
She was always told her lab tests were “normal” but after her insistence of stating she didn’t feel normal, she was finally given some thyroid medication even though it didn’t make a difference.
And this is where things get very interesting.
One of the primary reasons that she was never treated correctly is that her doctors were most likely using the “standard” reference range for determining if her thyroid was functioning optimally.
What they were failing to appreciate was her body’s remarkable ability to maintain serum levels of thyroid hormone despite missing 70% of her thyroid gland because they were focusing on standard reference ranges and not optimal reference ranges.
When you take a closer look at her thyroid lab tests, you can see some obvious issues:
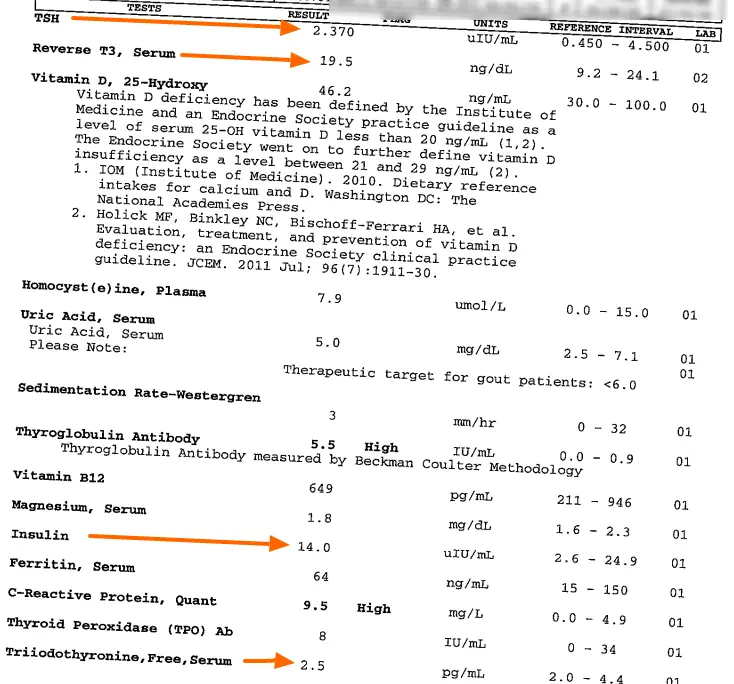
As you can see the majority of her lab tests do fall within the “normal” range with the exception of her CRP and thyroglobulin antibody levels.
But let’s go over the rest of the labs to help you understand the difference between “optimal” and “normal” and why she had great results when we finally interpreted these lab results correctly.
Her list of abnormal lab results includes:
- Suboptimal TSH: When not on thyroid medication optimal TSH levels should be < 2. This range is based both on anecdotal evidence as well as some newer studies (you can read more about why TSH levels can be inaccurate here).
- High Reverse T3: Indicating poor thyroid conversion. Reverse T3 should generally be < 15 for optimal thyroid function.
- Elevated thyroglobulin antibodies: Indicating a component of autoimmune thyroiditis contributing to poor thyroid function. You can read more about how to lower antibody levels here.
- High fasting insulin: Fasting insulin should be < 5. High levels contribute to weight gain and weight loss resistance and may make reverse T3 levels higher.
- Elevated CRP: Indicating inflammation is present in the body, optimal levels should be as low as possible.
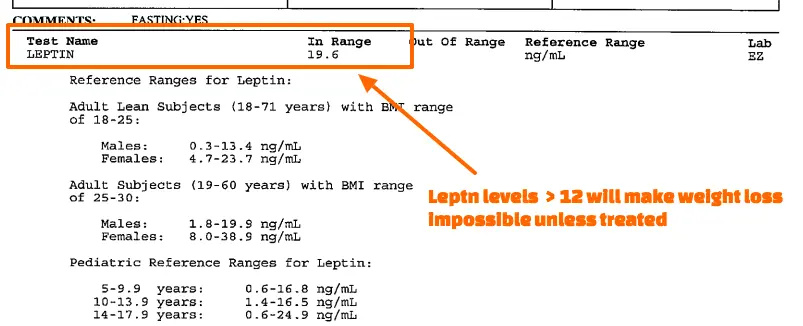
- High serum leptin levels: High levels make TSH less accurate, promote high reverse T3 levels, and also contribute to weight loss resistance.
Compare this evaluation to the previous notion that she was completely “normal”.
Does she sound or look “normal” to you?
Definitely not, and you may find yourself in this same situation.
Using these functional and optimal reference ranges, it’s easy to see that she is in fact NOT normal and that she has multiple hormone abnormalities contributing to both her thyroid symptoms and inability to lose a significant amount of weight despite eating a healthy diet.
So what is happening in her body and how does this explain her symptoms?
It’s hard to know for sure but based on what we are seeing here the likely answer is tissue-level hypothyroidism.
Tissue level hypothyroidism refers to a state where there can be adequate thyroid hormone in the body and bloodstream but that thyroid hormone is not responsive at the cellular level.
It’s also sometimes referred to as thyroid resistance (although this would be a form of acquired thyroid resistance and not a genetic version of thyroid resistance).
In this specific situation, thyroid medication was definitely the answer.
We know that based on her labs and her history of radioactive iodine ablation.
Even though she had some remaining thyroid function (approximately 30%) that tissue was not able to keep up with the demands of her body.
As a result, she experienced hypothyroid symptoms as well as weight gain.
Putting her on thyroid medication was definitely the answer but, unfortunately, her doctors used a low dose of the wrong type of thyroid medication.
Because her body had a hard time converting the T4 from levothyroxine into T3, she was never really able to meet the demand of her tissues or resolve her hypothyroid symptoms.
This persistent hypothyroid state then set the stage for her to develop other issues such as leptin resistance and insulin resistance as seen in her lab tests.
In a vicious cycle, these hormone imbalances then made her thyroid conversion worse and contributed to her high reverse T3 levels.
This scenario is bad by itself but it doesn’t stop there.
We also know that she has Hashimoto’s thyroiditis (she was diagnosed with this a long time ago) and even though she was placed on levothyroxine to try and treat her hypothyroidism, the underlying cause of her Hashimoto’s was never addressed.
We would then expect that over time she would see more damage to the remaining 30% of her thyroid gland tissue due to inflammation and destruction from her own immune system (the hallmark of Hashimoto’s).
This adds fuel to the fire mentioned above.
Ultimately, after years of struggling, she presented with these lab results which are what you are seeing now.
One final point worth mentioning is how reverse T3 impacts the function of thyroid hormone.
When we discuss serum levels of thyroid hormone we are more concerned about how much thyroid hormone is getting into the cells and not necessarily how much thyroid hormone is floating around in the serum.
“Normal” levels of thyroid in the blood do NOT mean that the tissues are getting enough thyroid hormone and this was certainly the case in this patient.
Her serum levels of free T3 and free T4 remained relatively preserved but she remained quite symptomatic despite this.
For this reason, the most sensitive measure of thyroid function in this patient is the relationship between free T3 and reverse T3, otherwise known as the free t3 to reverse T3 ratio.
And this patient is just screaming that she is hypothyroid with a ratio of 0.128!
The secret to diagnosing and treating many hypothyroid patients is this ratio because it will identify most hypothyroid patients when all other lab tests are “normal”.
This ratio can be helpful in cases of “normal” thyroid lab tests because it starts to become abnormal before any other thyroid lab tests make it outside of the normal reference range.
Treatment Plan + How to Approach a Patient Like This
The most important part of this patient’s evaluation is her management.
What I mean is how she was treated.
We can wax philosophical about her history, what is going on in her body, how she got there, and so on, for a long time.
But that doesn’t do us any good if we don’t fix it!
Many patients believe that if they can get all the “right” tests their doctor will finally treat them appropriately.
This rarely happens.
If your doctor isn’t willing to order the right thyroid blood tests then it likely means they don’t really know their purpose or how to interpret them.
And when it comes to getting results like this patient you really need to find someone who is willing to not only order and interpret the right tests but also provide appropriate treatment.
This means you need a thyroid-literate doctor.
If you are struggling to find one, you can use this resource to help.
So how do you approach a patient like this with multiple problems who is severely undertreated?
You have to take a comprehensive approach that includes treating the following areas:
- Hormones and prescription medications
- Supplements and botanicals
- Inflammation and autoimmunity
- Detoxification
- Diet and exercise (lifestyle factors)
- Stress Reduction
If these areas are not all addressed at some point then you’re not really treating the problem.
And this is a REALLY important point:
Make sure you don’t get what I call “thyroid tunnel vision”.
This is the idea that every problem that exists in your body is related to your thyroid and the solution is to simply change/increase/swap thyroid medication until you see a resolution.
Patients tend to fall into this category especially when they have extra weight to lose.
They wrongly assume that increasing their thyroid medication will result in significant weight loss.
At most changing or adding in thyroid medication will result in an average 5-10 pound weight loss.
If you are like many hypothyroid patients then you probably have more weight to lose than just an extra 5-10 pounds.
But I can assure you that the extra weight is almost always related to other factors.
Let me use this patient as an example to help illustrate this point:
Over a 9-month period of time, this patient experienced the weight loss you are seeing here as well as almost complete resolution in her low thyroid symptoms.
But what is interesting is that her hypothyroid symptoms were almost completely gone within the first 3 months of her treatment, but she only lost 20ish pounds or so during that time.
The remainder of her weight loss came in months 3 through 9 and without changing her thyroid medication.
She was able to lose this weight because during those months we focused on the other hormone imbalances that were a result of decades of low thyroid function but not directly due to her low thyroid state.
Yes, her initial low thyroid state set the stage for the weight gain but it wasn’t solely responsible for it which is why optifmizing her dose of thyroid medication resolved her symptoms but not all of her extra weight.
In this way optimizing your thyroid medication dose is necessary to lose weight but will not cause all of the weight itself.
And this is an important distinction that you should be aware of if you are trying to lose weight.
- Bottom line: When searching for a provider to help with your Hashimoto’s/Hypothyroidism make sure your provider also understands hormone imbalances that contribute to and potentiate weight gain and weight loss resistance.
T4 vs NDT & Reverse T3
*Note: this patient had success with Nature-throid, which hasn’t been available for some time, but you can always swap out its use for NP Thyroid or Armour Thyroid.
Why did this patient respond so well to Nature-throid when she didn’t respond to levothyroxine previously?
A big part of the reason has to do with conversion mechanics between T4-only medications and T4/T3 combination medications.
T4-only medications (like levothyroxine, Synthroid, and Tirosint) can work for some people but fall short in patients who have high levels of inflammation or insulin/leptin resistance.
One of the primary reasons for this is that the body converts T4 into either T3 (active thyroid hormone) or reverse T3 (inactive thyroid metabolite) and this conversion process is influenced by factors like inflammation.
If the body is in a state of inflammation then providing more T4 (in the form of thyroid medication) is like adding fuel to the fire, your body will take the T4 and turn it right into reverse T3 which blocks the action of T3.
You can bypass this problem by taking thyroid medications that contain T3 thyroid hormone.

Natural desiccated thyroid preparations contain a combination of T4 and T3 together. Each grain of Nature-throid contains approximately 38 mcg of T4 and 9 mcg of T3.
The benefit of adding T3 to T4 dosing is that the T3 can directly bypass the conversion pathway and has a direct action on the nuclear receptors of cells.
This means you don’t have to worry (*too much) about the conversion process because providing T3 thyroid hormone bypasses the necessity of thyroid conversion.
*This isn’t entirely true for everyone, though, because NDT formulations still contain more T4 than T3.
Generally speaking, the more inflammation, autoimmunity, stress, and hormone imbalances a person has the better the more likely they will need T3 thyroid medication.
Hopefully, this is making sense!
Beyond using the right type of medication, we still have to worry about the dose.
You can take the right thyroid medication but the wrong dose and not get any of the desired effects you are looking for.
This can be solved with self-titration.
Nature-throid Dosing and Self-Titration – How to Dose Your Medication
This patient was able to find her dose of Nature-throid by utilizing what is called self-titration.
If you’ve never heard of self-titration let me explain:
This is the idea of slowly but steadily increasing your dose every 10-14 days (depending on the patient) based on a combination of symptoms, lab results, and other factors (like resting heart rate/body temperature).
One major benefit of self-titration is that it allows for a slow and steady increase in thyroid hormone over weeks to months which then allows the body to adapt to thyroid hormone to minimize negative side effects that can come from using T3 medication.
While self-titrating it is a great idea to keep track of both basal body temperature and resting heart rate to help monitor the effectiveness of your thyroid dosing.
Monitoring these variables also helps to prevent accidental overdose which is something you definitely don’t want!
The patient in this case study titrated her dose up to a total of 2.5-3 grains of Nature-throid which is around 195mg.
Even though she did great on just pure Nature-throid, some patients need the additional T3 (Cytomel, liothyronine, or SR T3) along with their NDT.
As I mentioned previously, as she increased her dose many of her hypothyroid symptoms disappeared over the first 3 months or so.
Finding the Best Diet: AIP vs Nutritional Ketosis vs Other Diets
Diet is critical to treating and reversing Hashimoto’s and if used correctly it can also directly impact insulin and leptin levels.
What you need to realize, though, is that changing diet is typically not enough to normalize weight by itself.
Just like optimizing your thyroid medication, changing your diet definitely can help, but it must be accompanied by other therapies if you want to lose a significant amount of weight.
Many thyroid patients will lose some weight while trying various types of diets (usually in the range of 5-10 pounds) but this weight never stays off and they typically don’t reach whatever goal they are shooting for.
But this doesn’t mean diet isn’t important if you want to lose weight, the opposite is true.
I’ve written about the various types of diets you can use to help reduce antibodies and inflammation here which I would recommend checking out if you haven’t already.
In this particular patient, I started her on the autoimmune protocol (or AIP diet).
I generally don’t recommend this type of restrictive diet for most thyroid patients but this case is unique in that the patient had more than just one autoimmune disease (Hashimoto’s).
She also suffered from another autoimmune condition known as idiopathic thrombocytopenic purpura (1).
For this reason, I started her on the AIP diet and she did have a favorable response with a reduction of inflammation, an improvement in her platelet levels (impacted by her ITP), and a resolution in her thyroid symptoms.
While the AIP diet was effective in this case, it’s not necessary that everyone use it for Hashimoto’s or for weight loss.
In fact, it’s not even my preferred diet for thyroid patients (which you can find here if you’re interested).
It’s worth noting that prior to working with me, she had tried the ketogenic diet with minor success.
But, for the reasons I’ve mentioned in previous articles, low-carb diets like keto and carnivore may cause more harm than good for thyroid patients.
Using LDN for Autoimmunity and Inflammation
LDN, also known as low-dose naltrexone, is another tool that was used.
It was prescribed for several reasons:
- The fact that she had a history of multiple autoimmune diseases (both Hashimoto’s and ITP)
- Her joint pain
- Her insulin resistance
- Her high inflammatory levels
- Her issues with weight
She’s definitely a slam-dunk candidate as far as patients with Hashimoto’s go for using this off-label medication.
LDN can act as an immune modulator and help to reduce inflammation in some patients with autoimmune diseases.
It doesn’t work in every patient but I’ve found it to be particularly helpful in patients with autoimmune disease and chronic pain/chronic joint pain.
Studies have shown that LDN can be useful in various autoimmune conditions ranging from multiple sclerosis (2) to fibromyalgia (3).
In low doses, naltrexone may help to regulate immune function and balance multiple different neurotransmitters (4) which translates to symptomatic benefits in many patients.
LDN can also be used as a novel anti-inflammatory agent (5) which may help promote thyroid conversion and thyroid function overall.
In addition to all of these other benefits, naltrexone can help promote weight loss through hypothalamic changes (6) which mediate body set point and appetite triggers.
It should be fairly obvious why she was prescribed LDN because she fits just about every box you can in terms of potential benefits.
At one point during her therapy, she attempted to take herself off of the LDN and noticed a flare-up of chronic pain and joint inflammation, due to this she was placed back on the medication and has been on it since.
The Right Supplements to Help Thyroid Function
I can’t remember a single time that I treated a thyroid patient without recommending several different supplements.
Yes, they do add to the cost, but it’s my experience that they accelerate how quickly thyroid patients feel better.
And this situation was no different.
In this specific case, this patient needed and did well on the following supplements (she has been on various supplements through the 9 months of treatment but these have remained consistent):
- Vitamin B12 injections – For vitamin B12 deficiency (learn more about why B12 shots are better for patients with Hypothyroidism and Hashimoto’s here).
- Zinc + selenium – Zinc and selenium act to lower inflammation, balance immune regulation, and promote T4 to T3 conversion (helpful in patients with high reverse T3).
- Adrenal support – Cortisol dysregulation is common among patients with hypothyroidism and adrenal function should be treated along with thyroid hormone replacement.
- Probiotics – Decreased motility of the GI tract is common among hypothyroid patients due to thyroid action on peristalsis, GI dysfunction should be a cornerstone of treatment.
- Liquid Vitamin D + K2 drops – To replace low Vitamin D and to promote immune function. They can be used with or without vitamin K2.
Detoxing Endocrine Disrupting Chemicals
Another key to her success was spending some time on detoxification.
A lot of people are accustomed to thinking about detoxification as some sort of woo-woo buzzword that doesn’t mean anything and is only used by scammers.
The truth is that every single human being has built-in detoxification systems in the body to get rid of things we don’t want or need.
Sweat, stool, urine, and breath are the 4 biggest but your body can also eliminate toxins directly through the skin as well.
When it comes to thyroid dysfunction, the thing you should be most worried about is endocrine-disrupting chemicals.
These are chemicals, found in plastics, on receipts, liners of food cans, toys, cosmetics, etc., that are known to directly interfere with thyroid function at the cellular level.
Endocrine-disrupting chemicals, or EDCs for short, are everywhere nowadays, and it’s almost impossible to avoid them.
What’s worse is that some of them are fat-soluble and hide away in your fat cells (7) if they aren’t eliminated quickly enough.
Because they can be hidden away in your fat cells, they can be re-released into circulation as you start to lose weight.
Sometimes this re-release can impair your weight loss efforts and lead to plateaus unless they are actively removed or detoxed from your body.
Not everyone has to put a lot of energy into detoxification therapies, but there are some patients who benefit tremendously from doing so.
This patient was one of those.
She used weekly FAR IR sauna therapy in addition to high-intensity strength training and high-intensity aerobic interval training to promote sweating and toxin elimination.
Sauna therapy combined with this type of exercise promotes hormone balance, more weight loss, and helps eliminate waste through sweating.
Recap of Treatment, Therapies, & Expectations
Thyroid patients who are doing everything correctly should expect a steady 5 to 10 pounds of weight loss each and every month.
There will be some fluctuations in weight loss, though, because weight loss plateaus are not uncommon.
So even though your average weight loss will be 5 to 10 pounds per month, that number can vary slightly.
Many patients nowadays are looking for quick fixes or rapid weight loss.
They want to be able to lose 20 pounds in 1 month or less and believe that if something doesn’t work this rapidly it must not work at all.
This is the exact opposite mindset you want to have when it comes to weight loss.
Weight gain is a slow and steady process (usually) and weight loss is the exact same.
As long as you stay dedicated and consistent with your treatments, you will eventually hit your target weight goal over a period of time.
On average, you should expect it to take somewhere around 6 to 12 months depending on how much weight you have to lose.
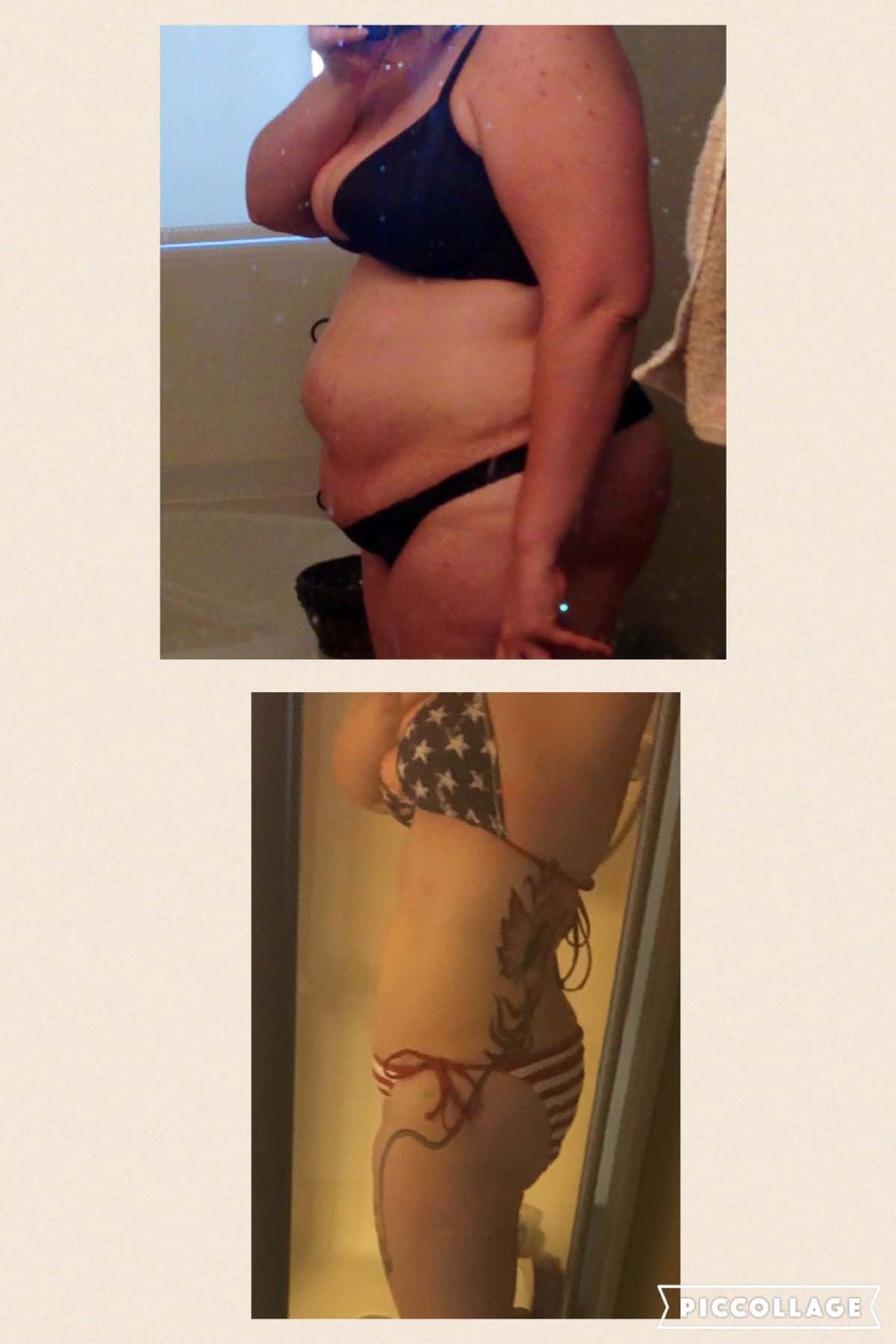
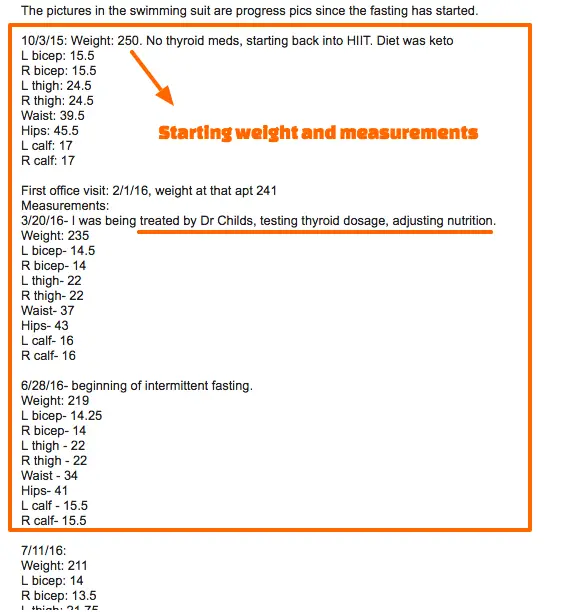
To give you a better idea of what this looks like, you can check out the results of this patient over time.
Let’s recap the initial treatment:
| Medications | Supplements | Diet | Detox |
|---|---|---|---|
| Nature-throid | Adrenal Support | AIP | Sauna |
| LDN | Zinc | Ketosis | HIST |
| Selenium | |||
| Vitamin B12 | |||
| Probiotic |
Her results after 3 months included:
30-pound weight loss, 27 inches lost, 80% reduction in symptoms, improvement in hormonal balance by blood tests.
After getting her dose of thyroid medication optimized, we then worked on other hormone imbalances including insulin resistance, low testosterone, and weight loss resistance.
You can see an image of those labs below:

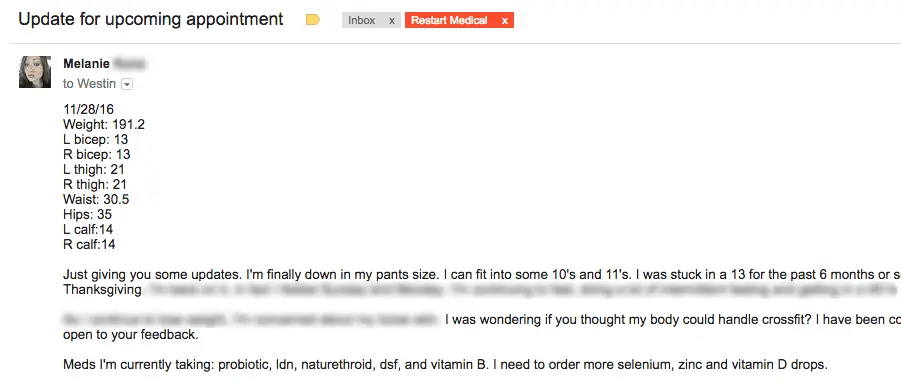
From month 3 to 9 she lost a fairly steady 5-10 pounds per month.
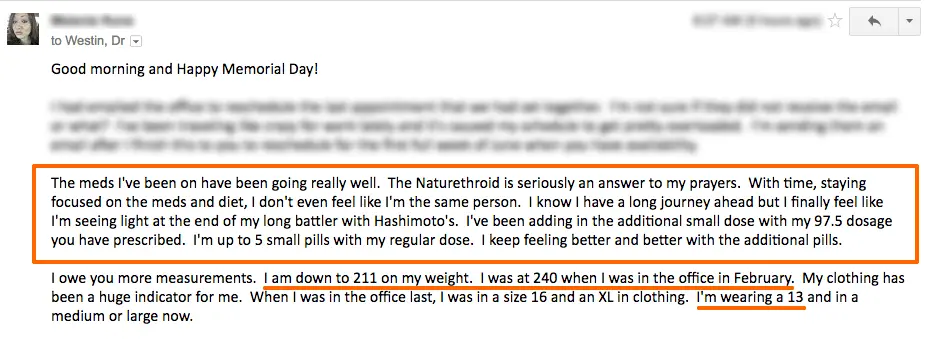
You can see her emails to me including her measurements and results below:
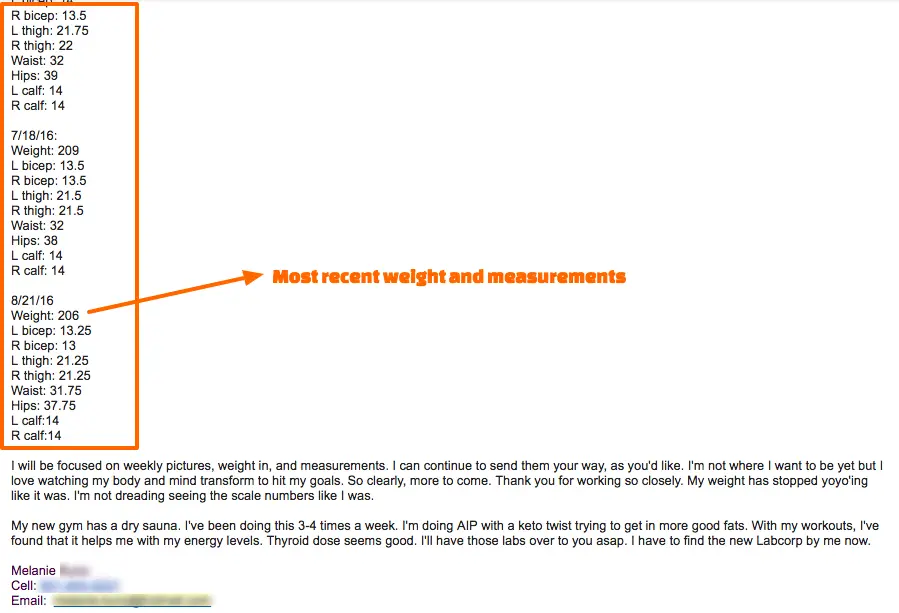
Update #2, 9-month results:
Final Thoughts
Why is it that so many thyroid patients continue to gain weight despite doing what they think is everything “right”?
To put it bluntly, they aren’t doing everything right.
But if you take a similar approach as Melanie, you can get the same results she did.
Now I want to hear from you:
Did anything in this case study surprise you?
Did it all make sense?
Do you see any similarities in your own personal journey?
Are you also struggling to lose weight despite changing up your thyroid medication or changing your diet?
Do you have any questions about this case study?
Leave your questions or comments below!
Scientific References
#1. https://www.mayoclinic.org/diseases-conditions/idiopathic-thrombocytopenic-purpura/symptoms-causes/syc-20352325
#2. https://www.ncbi.nlm.nih.gov/pubmed/21256121
#3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3962576/
#4. https://www.ncbi.nlm.nih.gov/pubmed/19041189
#5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3962576/
#6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3138366/
#7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2726844/





Hi Dr. Childs,
This all seems so complicated. I’m having trouble finding a starting point. I’m 35 years old and have been tired and run down my whole life. I struggle with my weight, thinning hair, cold extremities, PCOS, high blood pressure, scalp psoriasis, insomnia, I’m either so hot or so cold all the time, and the list goes on. I’m currently prescribed 50mcg of levothyroxine even though my labs have been normal? I had to really push to try something new. I also take B12 and D3 supplements For deficiencies. I’m not even sure if I’ve been tested for the right things though.
I have a TSH test result of 4.99. Hemoglobin A1C of 5.9.
Thyroid peroxidase <10 and a Thyroglobulin AB <20.
T4 FREE is .94.
I’m really frustrated trying to make sense of this all and I don’t know where my starting point should be. Any help or insight where to begin would be greatly appreciated!
Thank you!
Courtney
Hi Courtney,
It is quite complicated! That’s why this website exists 🙂 The first thing you want to do is start by getting a complete thyroid lab panel (and hormone panel, in your case). This will give you information that you can then act on. I would start here: https://www.restartmed.com/normal-thyroid-levels/
This is wonderful information. I have struggled with Hashimoto’s thyroiditis for a couple years. I find it very difficult to find a doctor to give me any helpful advice. I have tried levothyroxine and synthroid, both made me feel worse. I am now on Armour (per my request) and seeing results. My TSH went from 9.45, 4.14 within 8 weeks. My question is, should I continue to take supplements with this medicine? I purchased B12, vitamin D3 and iodine. I haven’t found a doctor that is truly helpful. I ask them what tests to run and medications to try based on my research. It’s been very frustrating. I just started intermittent fasting and am looking into doing keto as well. I’m only slightly overweight, but still not comfortable with myself. Feeling better though!
Hello. Thank you for the information in this article. Do you have any updates on the research from this case?
I am 39 years old and was diagnosed with Hashimoto’s 9 months ago. My doctor put me on Thyroid (NP) 60 mg daily And gave me a testosterone boost in the form of a pallet placed into the fat over my right hip. She assured me that I would start feeling the effects of it in 30 to 60 days and we schedule an appointment at that time for me to come back for a reevaluation of my bloodwork. When I went back, my blood work was normalized but I felt worse. I put on more weight, I was depressed, it had no energy still. My doctor adjusted the dose to a half tablet once daily but I continue to feel terrible.
I have tried doing a restrictive diet and wind up in tears most days out of frustration and extreme hunger. I have an amazing husband who gives me unconditional love and support through all of this, I exercise regularly, and I’m constantly looking for new information that might help me.
My question for you is, how do I find the right doctor? Are there questions that I should be asking? Is there a specific branch that I should be looking at other than endocrinologist? I live in England and have access to wonderful health care but I don’t know where to start. Any suggestions would be valued immensely.
Thank you for your time and consideration.
Hi Kathy,
The issue with treating thyroid patients is that I only ever heard from them if they are doing poorly or need some adjustments. What typically happens is that I set them on the right treatment, and it works, and I really don’t hear from them for months and months. I haven’t heard from this patient in a while but I have no reason to suspect that she is doing poorly given that she would have reached out if she was 🙂
You can find more information on how to find a doctor here: https://www.restartmed.com/thyroid-doctor/
Have you treated a type 1 DM? I have multiple auto-immune diseases and get “You should be in an endocrinology text book” but that’s it. So me-type1DM, PCOS, hashimoto and infertility, lipomas, joint pain. I am up to 288 lbs and work out regularly with ZERO loss. PLEASE HELP!
Hey doc what would you think if my TSH is 4.09 (0.32 to 5.04) , ferritin 77 (15 to 247), HemoA1C 5.9 (4.5 to 5.9), free t4 12.4 (10.6 to 19.7), free t3 3.87 (2.60 to 5.80), thyroperoxidase 72 ( should be under 35), vit D is well below and I’m on vit d drops.
I would love to have someone assess me the way this lady has been assessed and helped. Do you recommend a doctor who does this? I live in NC
Hi Asma,
I don’t know anyone in that area but you can use this resource to help you find someone: https://www.restartmed.com/how-to-find-a-doctor-to-treat-your-thyroid/
Dear Dr. Childs,
I just wanted to thank you for this and many other interestering and enlightening articles that have helped me tremendously.
Using your advice, I searched for a doctor knowledgeable about not only thyroid disease, but also other related hormones such as cortisol, insulin, and leptin. Not easy to find in Europe, for sure…!
I finally managed to find a doctor who diagnosed me with adrenal fatigue (a diagnosis not recognised by mainstream doctors in Europe) and put me on hydrocortisone for a few weeks before we switched me from levothyroxine to NDT + T3 (titrating it very slowly). Thanks to your advice, I also requested that not only insulin be tested but also leptin, and sure enough I had not only insulin resistance but also leptin resistance. I have now been on Ozempic for eight weeks and the difference in how I feel and look is amazing. All cravings are gone, I am able to eat a healthy diet, and I am even starting to lose weight for the first time in years. I was put on Ozempic rather than Metformin as the latter does not address leptin resistance, and I doubt I would have had the same results with Metformin…! But, if doctors only test blood glucose and insulin, you are likely to end up on Metformin as it seems to be the most used anti-diabetes drug and all doctors are familiar with it. If I had not read your articles, I would not have known about leptin and leptin resistance, and neither would my doctor as it was never discussed in medical school (not sure how it works today).
Even though my doctor is very knowledgeable compared to most other doctors, he has also learned a lot from your articles. Unfortunately, there are no laboratories in Europe offering rT3 testing, but based on my symptoms and your articles my doctor agreed to add T3 to NDT and it has also been a tremendous help. I now understand why I felt terrible on levothyroxine, while doctors told me I was “optimally treated” simply because my TSH was in range…
Hi Anna,
Glad you found the information helpful and thanks for sharing! I’ve talked to some patients in Europe who were able to get reverse T3 testing by sending it out to other countries. That may be an option for you as well but you’d have to look into it.
Dear Dr Childs
I have wanted to try LDN for a long time but I do not have a do y that can prescribe it as it is compounded.
Could you please let me know if you are able to prescribe it or a place where I can get it? I have not been able to feel any better for years and I think this might help. I also was diagnosed with Lyme about 14 years ago and have hashimoto and Interstitial cystitis. A lot of inflammation and pain. I never have been able to loose weight since I was young.
Hi Charlee,
I’m not seeing patients so I can’t provide it to you but pretty much any integrative or functionally trained doctor should have no issue prescribing it. You can learn how to find these types of doctors here: https://www.restartmed.com/how-to-find-a-doctor-to-treat-your-thyroid/
Dr. Childs,
I just celebrated my 52nd birthday and I feel like the email I received with this article was my “lightening bolt” gift. My journey began in earnest in 2007 with a 42 pound weight gain and 30% hair loss and multiple other issues occurring within a 90 day period. They threw me on Synthryoid doses and basically threw me away out of ignorance and lack of interest. My enlightenment came 100 pounds later in 2013 when, through my own research, I discovered Tirosint which was not known by ANY of the 13 doctors and 2 scientists that I had worked with the previous 6 years. The more regulated dose of T4 that Tirosint provided was a drastic improvement in helping brain fog and energy but nothing else changed. 5 years later and through dumb luck, I discovered a young but passionately curious and dedicated P.A. Whose Father is a chiropractor and he introduced me to the world of T3 and Reverse T3 lab levels and why they matter. It helped tremendously in some aspects but obviously not all. I won’t go into detail with the traumatic physical decline I suffered from 2016-2018 (I changed my entire life in 2018) but I found a natural medicine doctor when I moved back to Florida and had real hope again. Unfortunately, after the first year and some improvement including weight loss…I realized that all that was being pushed on me was a product line she was reselling that did nothing for me. I was having to point out the irregularities in my “normal” lab results to my doctor when she was telling me everything was “fine”. I have self-managed for the past 3 years and done all right. From 2018, I ate intuitively and lost 70+ pounds with Tirosint and Cytomel as my only intake (occasionally playing around with supplements) along with intermittent fasting (before it was cool and I even knew what that meant). I worked with a nutritionist and tried a modified Keto diet this year which had small success in helping me break my plateau of 202 pounds by 10 pounds….and it lasted a half a minute before Perimenopause showed up and kicked me into oblivion 6 months ago. My natural doctor wanted to throw me on to HRT regime and ordered another round of $1000 lab work (no insurance). I said “no.” And mentally “adios-ed” the relationship. I discovered Amberen and it made a HUGE difference after a couple of months in almost all the Perimenopause symptoms. Thyroid-wise, however, energy levels were frighteningly low and weight gain was being held off by almost starvation. (I know I know). Three weeks ago, I threw in the towel on EVERYTHING and gave up on medications, too, deciding I was better off with just the Amberen and slowly finding the right balance of natural supplements and products to heal. Now, 16 pounds later (as of this morning), ever increasing inflammation and reading this article about your patient who reads like my twin in many aspects (excluding updated lab work for me)….I realize that walking away from the medications was not a good long term solution. Since my body reacts very very very quickly to anything it is exposed to, I do not regret my decision. I would rather start back at ground zero…fresh…and building my optimal healing program…with you. Will you help me please? I am wanting to live and feel my best possible life. I am still open with just enough hope left for one more round of dedicated passionate persistence to succeed. Thank you for all that you are doing for all of us!! Heather
Hi Heather,
I am not seeing patients right now but I created this resource designed to help thyroid patients find thyroid-literate doctors near them that I would recommend you check out: https://www.restartmed.com/how-to-find-a-doctor-to-treat-your-thyroid/
Thank you:) I had already read that and looked up to an hour away in all directions and have received “crickets” in response. Same deal…pushing their products or someone else’s and when I asked if checking Reverse T3 levels (just as a no brainer basic test)…I was told by 2 of them that wasn’t a first step in the lab work evaluation process but one offered to add it. I’m going to continue for another couple of weeks on the supplements and if my body starts giving me its usual IN YOUR FACE hints…I’ll just find a doctor that will do as I ask and prescribe what I RECOMMEND unless they have really proven valid reasons why not. That’s our medical world we live in…and in South Florida…its all about Anti-Aging marketed under Naturopath and Integrative medicine. I will continue to consume everything on your website and if you have a recommendation on which of your products I may better benefit from as a starting point than the Amazon.com purchased supplments I’m taking….I would appreciate it! I ordered a couple of your products from them and they never arrived after 3 weeks but your folks were great about refunding my money! I’m happy to order directly from your website this time!
Hello! Thanks for sharing this case study. I am 39 and trying to lose weight. I am about 30 pounds overweight. I eat mostly Whole Foods, I lift weights 5 days a week and walk every single day. I am on 45 g of NP and feel great. The only issue is the weight is not budging. Any tips would be helpful.
Hi Adrianne,
You can find a lot of tips and tricks to help you lose weight here: https://www.restartmed.com/lose-weight-hypothyroidism/
Hi Dr Childs this is a fascinating article to me. I’ve been diagnosed with hypothyroidism for over 15 years now. I think I’ve had it since I was about 18 and I’m now 44 years old. Since being diagnosed I’ve not had one normal range blood test. I’ve been as heavy as 300lbs and I’m now stuck at about 250lbs and have been for 3 years. This is despite basically starving myself and adding exercise and weight training. I also have fibromyalgia. All my GP does (I’m here in the U.K.) is increase the levothyroxine and it’s currently at 225mcg. I’ve brought some T3 but I’m concerned about taking it and how much to take. I just want to get some sort of healthy life back. Can you help or suggest anything? Thank you.
Hi Emma,
I’m not able to provide medical advice but I would suggest reading through these weight loss case studies to give you a better idea of what may be necessary:
https://www.restartmed.com/weight-loss-naturethroid/
https://www.restartmed.com/weight-loss-hypothyroidism-success/
https://www.restartmed.com/diabetes-reversed/
https://www.restartmed.com/thyroid-weight-loss/
https://www.restartmed.com/victoza-weight-loss/
https://www.restartmed.com/adding-t3-ndt/
hello, my son is 11 years old 2 years ago he was diagnosed with ITP trombocytopenia and hashimoto with only antibodies present and T3 and T4 in normal values, but with visibly enlarged thyroid on his neck. few months ago on check up he went from hashimoto to hyperthyroidism and doctor prescribed him Tiastatin. He is losing weight and is at risk of triggering ITP as Tiastatin is lowering his trombocyte levels. i cant get his doctors to work together or to consider both things hematologist told us to treat thyroid and see what happens with ITP and endocrynologist just gave this medicine and told us to consult hematologist. Basically nothing. also there is no talk about possible inflamation, gut health issues or anything beyond treating immediate condition. i feel he did not get appropriate treatment two years ago and he is not getting a lot of help now either and we are looking where to turn to or what research we can do ourselves and than try to present it to his doctors, or find different doctors entirely.
Dr. Childs,
Over the years, I have benefitted hugely from your advice. I know you are a proponent of liraglutide and similar drugs for insulin resistance and weight loss. But since these drugs raise insulin secretion to lower blood glucose levels, I wonder if you consider them to also raise rT3 in patients on levo or NDT?
Hi Anna,
My thoughts and opinions have changed on a lot of things over the years, including on GLP-1 agonists. If you want to see my most current thoughts, please see this article: https://www.restartmed.com/glp-1-agonists-and-weight-loss/
I am a hashimoto patient, inflammation
Is a big problem, along , with all of the other triggers joints,vision,memory, brain fog, on on. I’m with a new dr again, she allows me 20 minutes. I was shocked. She keeps saying my blood work is normal. It can’t be.
Wondering if you had a case study, would like to join. I also can fall asleep, if I eat certain foods, without even knowing it. Allergies to almost all medicines. Next dr appointment is in March 2024.
Weight 230
Shirley
ppmspirate1@yahoo.com
Hi Shirley,
I’m not seeing patients but you can use this resource to help you find a better thyroid doctor: https://www.restartmed.com/how-to-find-a-doctor-to-treat-your-thyroid/
It’s not worth wasting your time on doctors that aren’t willing to work with you because, in the end, you are the one that suffers (not them).
As I read this case study, it felt like they were talking about me. I have done almost all of this however, I have seen multiple doctors and they will not prescribe T3, nor neltexone, nor will she change my medication to something other than levothyroxine. It’s these difficulties that I believe have kept me from losing the weight. It’s so frustrating to know what help you need and unable to find a doctor that is willing to help.
Hi Danielle,
It is certainly frustrating to be in that situation.
Part of getting the treatments that I recommend is finding the right type of doctor and that usually means looking outside of the insurance model. You can sometimes get lucky with a conventional primary care doc or endo who is willing to prescribe these treatments but, most of the time, they aren’t willing.