- Hormone imbalances, not calories, drive weight loss resistance. This patient lost 21 pounds of pure fat in just one month by treating insulin resistance, low testosterone, and thyroid issues, not by eating less.
- Elevated fasting insulin levels literally shut off your body's ability to burn fat as fuel. Getting insulin below 5 is essential if you want to lose weight and feel good with hypothyroidism.
- Expect steady 5 to 10 pounds of fat loss per month when you're doing thyroid treatment correctly. Fast weight loss often means you're losing muscle too, and that slows your metabolism long term.
- Combining hormone replacement with intermittent fasting, supplements targeting specific deficiencies, physical therapy, and stress reduction works together in ways that no single approach can achieve alone.
- If you've struggled with yo-yo dieting and gastric surgery, you likely have thyroid resistance and elevated reverse T3. You need comprehensive hormone balancing and not just higher doses of the same medication that didn't work before.
Are you frustrated with trying to lose weight with your sluggish Thyroid?
In this post, I am going to go “behind the scenes” of what I do inside my clinic and show you how balancing your hormones is the KEY to weight loss success in patients with Hypothyroidism (or any medical condition!).
Note: This is an actual patient from my office, and this is what THIS patient needed for her weight loss. I don’t recommend you use any of the therapies listed below for you personally unless you are evaluated by a Doctor.
Let’s jump in:
This patient presented to me with multiple symptoms and was looking to lose weight and balance her hormones.
She is 69, a mother of 3 kids, and has been struggling with her weight ALL of her life.
Her primary goals of treatment:
- Lose weight (100 pounds ideally)
- Feel better and have more energy
- Improve her sleep
Throughout her life, she tried numerous diets including the HCG diet x3 (she lost 40 pounds the first time, 20 the second, and 10 the last time) and different yo-yo diets throughout the last 20 years…
**Update: Patient now has lost a total of 60 pounds which is 20 pounds lower than what she was able to do with her gastric bypass surgery – more info at the end of the article including testimonial**
- My Thoughts: Chronic yo-yo dieting leads to increased levels of Reverse T3 and Thyroid resistance. It can also lead to Leptin resistance. NEVER do this kind of diet!
Dieting & How It Affects The Thyroid
Before she came to see me she was most recently seen by another “holistic” provider who put her on a ton of supplements – but she never actually lost weight.
- My Thoughts: Stay clear of providers who only want to put you on a diet or supplements to help you lose weight. Weight loss is a problem with your hormones, NOT calories.
As part of trying to lose weight, she had a lap band surgery, and with the lap band, she was able to lose 40 pounds initially – but eventually plateaued and over the last several years put all of that weight back on + 15 pounds.
Her weight has been a huge source of stress in her life and is taking a toll on both her self-esteem and her health. She has elevated blood pressure, high cholesterol, and diastolic dysfunction stage II.
A brief review of organ systems:
Gastrointestinal tract: She has daily diarrhea – and has for many years (ever since her surgery).
Energy Levels: 4-5 out of 10 on good days. (10 being “optimal” energy levels)
Sleep: Suffers from insomnia, is unable to “slow down her mind” at night, and requires the TV on at all times to fall asleep.
Exercise: She gets on a bike daily for 30-40 minutes
Pain: She suffers from chronic pain in her neck, back, and both knees.
Diet: Consists of Salads every day, very little fat, and high protein in the form of lean meats.
- My Thoughts: Low-fat diets with lots of low-intensity exercises do NOT help with weight loss. For more information, you can see my recommendations on diet and exercise for those with hypothyroidism here.
After our initial consultation, I sent her for a Comprehensive Functional Blood Chemistry Panel, which I will go over below:
Comprehensive Functional Blood Chemistry Analysis
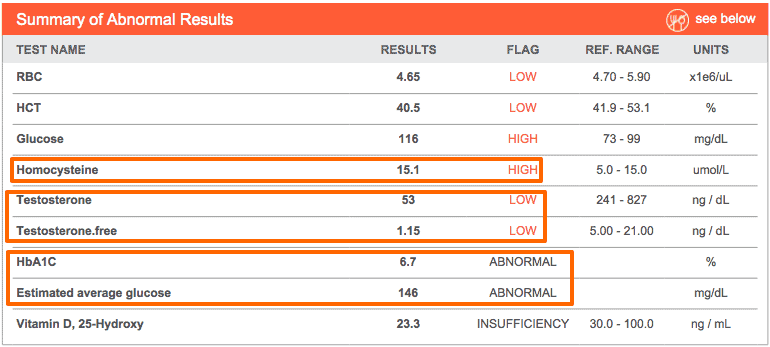
The following labs were “out of range” by the laboratory standards, for the tests that were “in-range” but suboptimal we will go over below (including thyroid studies):
Elevated Homocysteine – An inflammatory marker and high levels are associated with an increased risk of developing heart disease.
Low testosterone – Women need testosterone too! Low levels of testosterone are associated with a depressed mood, inability to lose weight, and inability to create and maintain lean muscle mass (lowers overall metabolism of the body).
Elevated blood sugar – By conventional standards, she falls into the Diabetes range (we will go over this below).
Low Vitamin D – Low levels of Vitamin D make hypothyroidism worse, and low levels are associated with an increased risk of developing autoimmune disease.
Now for going over the more subtle (but probably more important), functional lab tests that are in the “normal range” but still sub-optimal.
Cholesterol
This patient was on a Statin medication (Simvastatin) when she came to see me, which explains her lowish LDL.
In this patient, I’m more interested in her high triglycerides and HDL. This ratio can act as a surrogate marker for insulin resistance (which she does have) and when combined with elevated homocysteine makes me worried about her overall risk of developing heart disease (1).
She is also suffering from Diastolic heart dysfunction and High blood pressure – which can stem from insulin resistance (2).
Luckily these conditions can be reversed VERY quickly – in fact in as little as 1-2 months with intensive diet and exercise routines.
*Note: If a patient doesn’t have a history of heart disease (previous heart attack), the data does not necessarily support the use of Statin medications – Statins have been associated with an increased risk of developing diabetes (3), muscle damage (4), and are associated with an increased risk of developing breast cancer (5).
Blood Sugar and Insulin



Insulin resistance and blood sugar issues are VERY common in hypothyroid patients.
As you can see above this patient has Insulin resistance AND elevated blood sugar which puts her in the range of Type II diabetes mellitus.
Her insulin is also elevated – which is a huge part of the reason she is unable to lose weight.
Recall that with high levels of insulin (I use 5 as a cutoff) your body will store all calories you consume as FAT. Insulin literally turns off the enzymes in your body that allow you to burn fat as an energy source.
In this patient, a FASTING (12-hour) insulin level of 23.8 will be a huge issue for her and explains her inability to lose weight – especially when combined with her other hormonal imbalances.
As you can see her Uric acid is also elevated – this tells me that her liver has a problem metabolizing fructose (6) and that she is likely consuming extra sugar in her diet.
Thyroid Studies
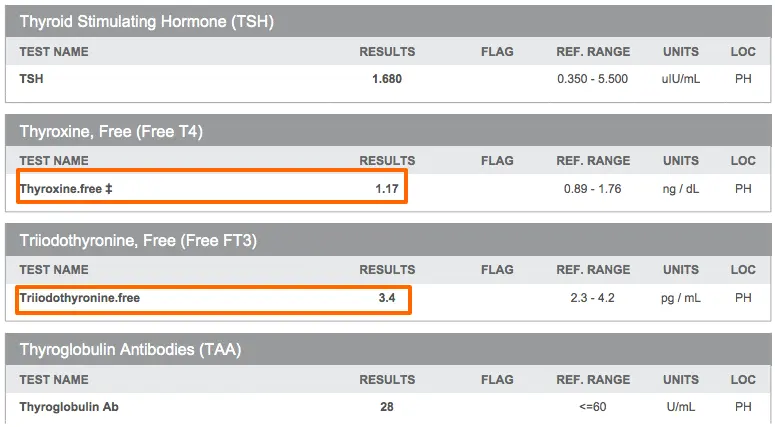


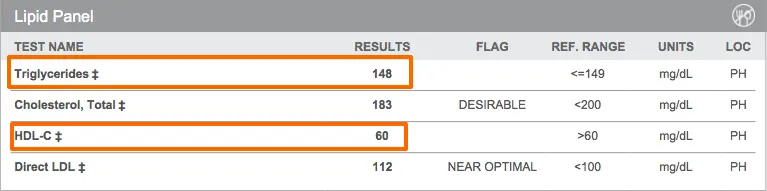
These thyroid studies definitely fall within the “normal” range by the definition of the labs.
Despite that, this patient suffers from multiple hypothyroid symptoms and also has several other signs of hypothyroidism including low resting pulse, decreased body temperature, and symptoms of hypothyroidism.
Because of these findings and because insulin resistance is associated with low levels of T3 in the serum (7) and a hypothyroid state – I treated her with thyroid hormone.
As you can also see, her free T4 and free T3 levels are suboptimal – both falling within the lower first and second quartile of the reference range.
In addition, her Reverse T3 is elevated which is causing an inappropriately increased free T3 level (8).

In tricky cases, you can also look to Sex Hormone Binding Globulin to assess liver tissue levels of thyroid hormone.
Low SHBG is associated with tissue-level hypothyroidism, and tracking SHBG levels (9) with treatment can be used to get an idea of how much Thyroid Hormone is actually getting to the target tissues.
In this case, you can see that low levels of SHBG are consistent with tissue-level hypothyroidism and high levels of reverse T3.
Note: It’s unclear to me whether her insulin resistance caused her hypothyroidism or if her hypothyroidism contributed to her insulin resistance – but in either event, both need to be treated!
Iron Studies
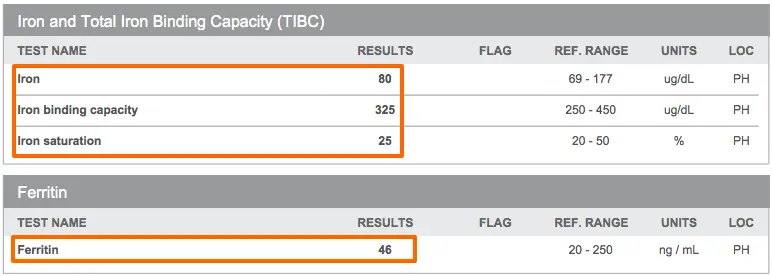
Iron is critical to measure because low levels are associated with decreased thyroid function (10).
In this patient, you can see that her levels are “normal” but they all fall within the lower portion of the reference range.
Through treating hundreds of patients I’ve found that optimal thyroid function happens when Ferritin is around the 70-80 range.
Vitamin B12

Vitamin B12 deficiency (11) is a BIG deal and often missed by many providers who aren’t looking for it.
Absorption of B12 is dependent upon hydrochloric acid, and with hypothyroidism, stomach acid is generally low – this results in decreased absorption of Vitamin B12 in many hypothyroid patients.
In addition – subclinical vitamin B12 deficiency is VERY common (12) and often undiagnosed.
Because of this, I treat patients with vitamin B12 if they have: Low or mid-range serum B12 levels, an MCV > 92 on red cell analysis, or elevated homocysteine levels.
This patient has several of these lab values so I opted to treat with methylcobalamin injections to saturate the tissues with B12.
Diagnoses
After going over the results with her above, and assessing her symptoms she ended up with the following diagnoses:
- Thyroid Resistance, Hypothyroidism
- Insulin Resistance, Type II Diabetes Mellitus
- Low Testosterone
- Adrenal Fatigue
- Insomnia
- Diastolic Heart Disease
- Iron Deficiency
- Chronic Diarrhea, with multiple nutrient deficiencies
- Vitamin B12 Deficiency
- Vitamin D Deficiency
- Hyperlipidemia
- Hypertension
As a side note:
Don’t let this list of symptoms and diagnoses scare you.
These are just names of her conditions, what we really care about is WHY.
In this case, my suspicion is that something like this occurred:
Her history of multiple episodes of recurrent yo-yo dieting led to her thyroid resistance. In an attempt to lose weight, her gastric bypass likely led to malabsorption of iron and B12 with chronic diarrhea, further worsening her hypothyroidism.

Her insulin resistance and Hypothyroidism are likely contributing to her high blood pressure and abnormal cholesterol panel.
High levels of stress lead to adrenal fatigue and symptoms of insomnia, extreme fatigue, and food cravings.
Following this logic, our treatment should be aimed at reversing these conditions (which I will go over below)…
Treatment
Here I will go over the treatment that this particular patient needed, and then give some follow-up thoughts on why I did what I did.
Please remember that this treatment is specific for THIS patient!
Do not take any treatment recommendations and apply them to your health. Every patient needs to be treated differently because no two patients are alike.
How to use Functional Medicine for Optimal Treatment:
Hormones and Medications:
In her case, I replaced hormones that were identified as being suboptimal with her blood work:
- Armour Thyroid
- Bio-identical Testosterone (In an organic base)
- Phentermine (To be used with fasting protocol)
Even though it is likely that her thyroid and testosterone are both low due to insulin resistance, I still prefer to treat patients in this position because they will often get faster results and will feel better quicker.
My goal is to always reduce medications whenever possible, so if her hormones balance out after treatment I will attempt to decrease her dosing of these medications.
Because of her age and symptoms, I started with 30mg of Armour Thyroid (She is currently on 60mg and doing well).
Supplements:
Her supplements were targeted to her comprehensive functional chemistry panel:
- Zinc + Selenium to boost thyroid conversion, 2 capsules daily
- Vitamin B12 injections once per week x10 weeks (Methylcobalamin)
- Vitamin D3 10,000 IU per day
- Adrenal Support, 2 capsules twice per day
- Liquid Iron 1 Tsp per day
- High potency probiotic 1 sachet per day
To learn more about what supplements I use and why I use them I encourage you to check out this post here.
Most of these supplements were targeted at specific deficiencies in the blood work, the only exception being adrenal support.
The probiotic was used to help balance out intestinal dysbiosis from the gastric band and chronic diarrhea.
Physical Work:
This patient had significant pain and multiple tender points along her neck, mid back, and lower back.
My suspicion is that these tender points were potentiated by low levels of thyroid hormone.
Because of this, I recommended soft tissue physical manipulation and low-intensity vibration therapy on a weekly basis, in addition to cranial sacral work.
Fasting Routine:
Elevated insulin levels (especially in the fasted state) contribute to weight loss resistance.
Unfortunately, fasting can be tricky in patients with Hypothyroidism. Especially when most Hypothyroid patients also suffer from adrenal fatigue.

As you can see below she dropped her fasting insulin from 23.8 (12-hour fast) to 10.3 (24-hour fast).
Our goal is to get insulin levels below 5 but each time her body drops her insulin level it will become more sensitive and subsequent fasting episodes will further drop her insulin level.
Before and after each fast I checked her percent fat mass, muscle mass, and water weight.
Stress Management:
Emotional and Stress reduction therapies are critical to managing both weight loss and overall health.
This patient had a history of being unable to sleep due to her mind being constantly “turned on” at night.
Because of this, I had her practice a combination of biofeedback, mindfulness, and guided meditation to lower stress levels and help her sleep.
This therapy was done in the office.
Dietary changes:
Diet is critical to weight loss, but by itself isn’t always enough.
In this case, I started the patient off on a gluten-free, dairy-free, soy-free, and sugar-free diet.
Her diet was high in healthy fats, nutrient-dense, and filled with real whole food.
She met with my health coach/nutritionist weekly to help her integrate new food groups and menu plans into her daily life.
Exercise:
Due to her untreated hypothyroidism and adrenal fatigue, I started her off on low-intensity exercise.
After 1 month I started her on HIIT – in the form of 10-15 minute bursts once per week.
Detox:
Many hypothyroid patients need to eliminate endocrine disruptors from their bodies in order to improve their thyroid function.
In addition, as the body starts to burn fat stores for energy, the fat cells can dump excess fat-soluble toxic compounds into the body.
This is especially important during fasting routines when the body burns TONS of fat for energy.
I had this patient do weekly FAR infrared sauna therapy for several reasons:
- Activate heat shock (13) proteins in the liver for detoxification
- Help the body burn extra calories (14) for weight loss
- Help eliminate toxins through sweating
- And help the body relax by reducing cortisol levels (15)
Results
In using this multi-faceted functional medicine approach to care, the results can be very impressive.
This patient was able to improve almost ALL of her symptoms within 1 month of treatment – which I will go over below:
Weight loss:
*Note: Weight loss is measured in percent fat mass lost by impedance analysis of the body. Note that the total weight did drop more than just percent fat mass, but I consider this a more accurate measure (along with body measurements) of fat loss.
Week 1 – 5 pounds of fat mass lost
Week 2 – 7 pounds of fat mass lost
Week 3 – 4 pounds of fat mass lost
Week 4 – 5 pounds of fat mass lost
Total lost over 1 month of treatment: 21 pounds of fat mass
This weight was lost without losing any muscle mass and without persistent calorie restriction.
Insomnia:
By the end of week 2, this patient was sleeping a full 8 hours through the night and was able to sleep without turning on her TV at night for background noise.
In her case, I believe her insomnia was due to a combination of adrenal fatigue and some degree of undiagnosed anxiety.
Both were improved with hormone balancing, supplements, mindfulness, and physical work.
Energy:
Current Energy levels = 8/10, an increase from 4-5/10
Energy levels are subjective but can be used as a general “marker” for how well her thyroid and adrenals are functioning.
Chronic pain:
At the end of 4 weeks of treatment, her pain had almost completely resolved, and at this point, she no longer has back pain.
In this patient, I believe her pain was due to her elevated insulin levels and anatomical changes which were dealt with by physical work and a fasting regimen.
Final Thoughts
This patient is still undergoing treatment with me, and I will continue to update her results from time to time.
At this point, I believe she will continue to lose fat mass and improve her energy over the next 4-6 months.
I wanted to use this patient as an example to show what a comprehensive, functional medicine approach to care actually looks like.
Many people are stuck in the conventional medicine mentality and they wrongly believe that changing up their medication from Synthroid to Armour thyroid will solve all of their health problems.
This couldn’t be further from the truth.
In many cases switching medication will help symptoms, but it won’t be enough by itself.
Whenever possible your doctor should attempt to go after the primary cause of your symptoms and reverse that.
Updates:
The patient is now down a total of 60 pounds (20 lower than she was able to achieve after her gastric bypass) continuing her fasting protocol and adding in a GLP-1 agonist for her leptin resistance.
Her weight loss plateaued at around 50 pounds of weight loss, so we checked her leptin level:
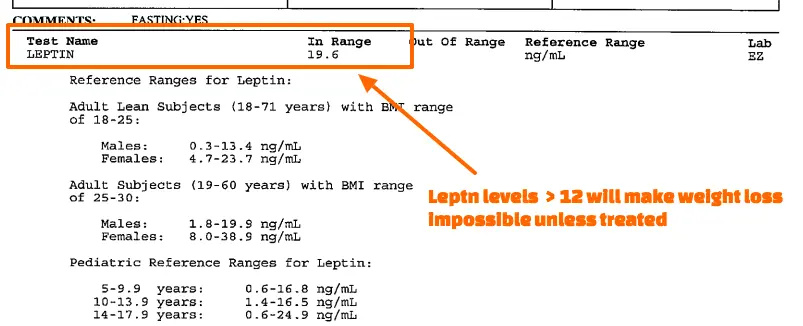
You can see from the above that her leptin levels are > 12 indicating that she has leptin resistance.
Even though she was able to lose weight initially this was the cause of the plateau at around 50 pounds.
After adding a GLP-1 agonist to her regimen she was able to lose another 10 pounds total.
You can find her review and testimonial below:
I want to hear from you!
What kind of treatment have you received for your thyroid? What worked and what didn’t? Is your doctor using a similar approach to treat you?
Let me know in the comments below!
Scientific References
#1. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2664115/
#2. http://www.ncbi.nlm.nih.gov/pubmed/7512468
#3. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4118294/
#4. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2849981/
#5. http://www.ncbi.nlm.nih.gov/pubmed/23833125
#6. http://diabetes.diabetesjournals.org/content/62/10/3307.full
#7. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3647563/
#8. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1628409/
#9. http://www.ncbi.nlm.nih.gov/pubmed/1618999
#10. http://www.ncbi.nlm.nih.gov/pubmed/16500878
#11. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3257642/
#12. http://www.ncbi.nlm.nih.gov/pubmed/16537043
#13. http://www.ncbi.nlm.nih.gov/pubmed/11741035
#14. http://jama.jamanetwork.com/article.aspx?articleid=360118
#15. http://www.ncbi.nlm.nih.gov/pubmed/3788622





