- Switching between thyroid medications is not as simple as a one-to-one swap because different thyroid hormones have different biological activities.
- The conventional thyroid conversion chart used by most doctors tends to be overly conservative, which often results in patients being underdosed when they switch medications.
- When converting from T4-only medication to NDT, you need to account for both the T4 and T3 components in NDT to avoid feeling worse after the switch.
- T3 thyroid hormone is roughly 3 to 4 times more potent than T4 on a microgram-for-microgram basis, which is why even small changes in T3 dosing can make a big difference in how you feel.
- If you are switching thyroid medications, work with a doctor who understands these conversion ratios and is willing to adjust your dose based on both your labs and your symptoms.
Are you taking one type of thyroid medication but considering switching to another?
If so, then this is the article for you.
The truth is that while many thyroid medications contain similar ingredients, the switching process is not as straightforward as you might think.
We are going to talk about switching from T4-only medications (levothyroxine & Synthroid) to NDT medications (Armour thyroid, NP thyroid, etc.), and also how to convert between T4-only to T3-only and vice versa.
Note: want an easy way to get your medication converted? Try my free thyroid medication calculator. It combines all of the information on this page in an easy-to-use tool.
Conventional and Conservative Thyroid Conversion Chart
This may surprise you, but there are several different thyroid medication conversion charts.
The reason for this has to do with the relative power or biological activity of each thyroid hormone.
It’s hard to compare the biological activity of various thyroid hormones because each thyroid hormone plays a different role in the body.
But by using some research and basic math, we can create rough equivalents that we can then use to make recommendations when converting from one thyroid medication to another.
To start, I’m going to include 3 basic charts for you to look at.
The charts exist on a spectrum from conservative to aggressive.
What you are probably already accustomed to is what I will refer to here as the conventional or ultra-conservative thyroid conversion chart.
This is the chart that you will see in major pharmaceutical textbooks and the chart that most doctors are probably using.
There’s one big problem with this chart:
It isn’t necessarily the best and using this chart does result in underdosing in many patients.
Why?
Well, because most doctors would rather underdose you than overdose you.
The more aggressive the conversion you use, the more likely you are to experience symptoms, even if this rate is probably only around a few percent (2-3%).

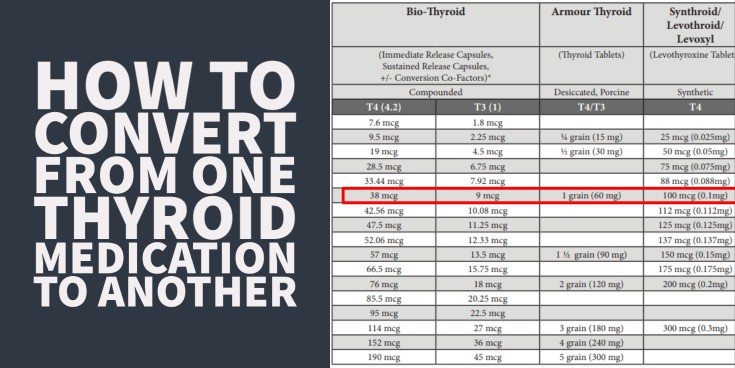
The first thing you will notice from this chart is that it includes information that allows you to convert from T4-only medication to NDT medication to T3-only medication to synthetic T4 + T3 combinations.
What you might not realize is that these conversions don’t really make a lot of sense once you start to break them down.
The information suggests that 1 grain of NDT (which is 38mcg of T4 and 9 mcg of T3) is equal to 100mcg of T4 only, which is equal to 25 mcg of T3, which is equal to 1 grain of synthetic T4/T3 (which contains 50mcg of T4 and 12.5mcg of T3).
Let’s break this down by looking at a couple of these individually.
Based on the numbers here, the chart suggests that T3 is about 4x more potent than T4 as a thyroid medication.
This tracks somewhat closely with my own real-world experience, but is still slightly more conservative than what I see in real life.
They are suggesting that 25mcg of T3 is equal to 100mcg of T4.
25 times 4 would be 100mcg so if you are taking 25mcg of T3 you can consider that to be 100mcg of T4 equivalents.
Now let’s look at the NDT to T4 conversion.
The chart suggests that 1 grain of NDT (which is equal to 38 mcg of T4 and 9 mcg of T3) is equal to 100 mcg of T4.
If we multiply T3 by 4 (remember we already found that T3 is about 4x more potent than T3) in NDT, then we get that the 9mcg of T3 found in 1 grain of NDT is equal to 36 mcg of T4 equivalents.
Then, if we add the 38 mcg of T4 found directly in the NDT in addition to the 36 mcg of T4 equivalents from the T3 component, we get a total dose of 74 mcg of T4 equivalents in 1 grain of NDT.
Do you see the problem here?
The chart suggests that 1 grain of NDT is equal to 100 mcg of T4, but we just found that NDT only contains about 74 mcg of T4 equivalents!
Using this chart will result in underdosing by about 25% if you use it to transition from T4 to NDT!
That is just one of the issues with the standard conversion chart, but there are plenty of others as well.
The next most obvious problem is that the chart suggests that 1 grain of NDT (which, again, contains 38mcg of T4 and 9 mcg of T3) is equal to 1 grain of synthetic NDT, which contains 50mcg of T4 and 12.5mcg of T3.
What?…
How can 38 mcg of T4 and 9 mcg of T3 be equal to 50 mcg of T4 and 12.5 mcg of T3?
It doesn’t make any sense, and this is part of the reason that I really don’t suggest using this standard conversion chart.
Does it have value?
Of course, but I find it’s best used as only a very rough estimate to help you get on track.
But don’t be surprised if you use this chart and find that your hypothyroid symptoms return as you transition.
This chart leans heavily in favor of T4, which is why this may occur.
T4 tends to have much less biological activity than T3 (1), so if you use more T4, you will have a smaller effective dose of thyroid medication.
")
I’ve seen a number of patients who use this chart and then are surprised when they find that their TSH increases after the switch.
Of course, this will happen if you are switching to a lower effective dose of thyroid medication!
It doesn’t matter if you are switching from T4 to NDT or NDT to T4 or any combination.
If you provide your body with a lower effective dose of thyroid hormone, then you will feel it, and you will see a rise in your TSH.
Are there other, more effective charts to look at?
Yes! And we are going to dive into those next.
Updated Thyroid Conversion Chart Based on Newer Studies
What’s interesting is that newer studies have suggested that the conventional chart (the one I listed above) is probably not as effective as we once thought.
Most physicians who use it are aware of this but there aren’t really many other options to go by so they use it anyway.
More recently, however, there have been newer studies that suggest a newer conversion schedule based on the results of these studies.
This study (2), for instance, compared patients taking NDT and T4 and looked at how these medications influence thyroid labs.
They concluded, based on the results of their study, that there is a better way to convert between NDT and T4.
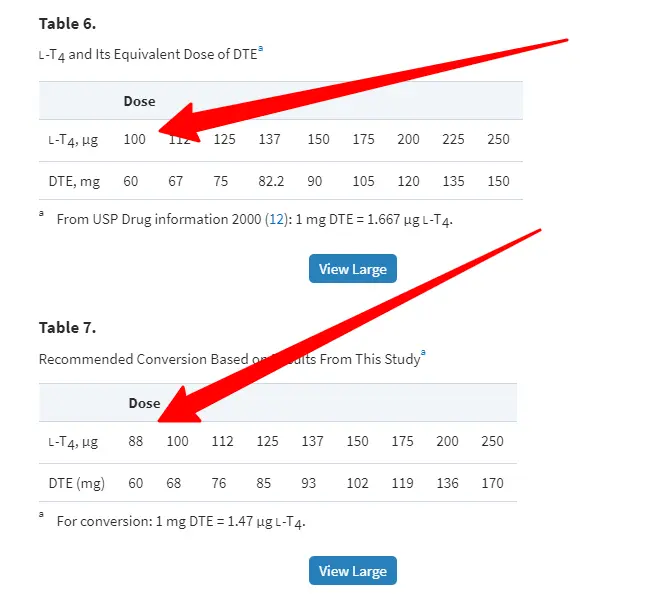
Instead of suggesting that 1 grain of NDT is equal to 100 mcg of T4, they found that 1 grain of NDT is equal to 88 mcg of T4.
So, this pushes their chart away from the T4 bias that exists in the original chart that I showed.
They also created this information based on studying patients taking both T4 and NDT and looking directly at their lab tests.
One of the downsides to the original chart that I showed is that it is purely theoretical and based on what we believe is happening.
This chart is better, in my opinion, because it is founded on real results and real patients.
You can find a more complete version of the chart that I created below for you (based on their results):
| Armour Thyroid | NP Thyroid | Synthroid (T4 only) | Cytomel (T3 only) |
|---|---|---|---|
| 30 mg | 30 mg | 44 mcg | 12.5mcg |
| 60 mg (1 grain) | 60 mg (1 grain) | 88 mcg | 25mcg |
| 90 mg | 90 mg | 132 mcg | 37.5mcg |
| 120 mg (2 grains) | 120 mg (2 grains) | 175mcg | 50mcg |
The study did not include conversions for T3 but I extrapolated from the original table which said that 100 mcg of T4 was equal to 25 mcg of T3.
If that is true, then 88 mcg (the new 100 mcg equivalent in this table) is also equal to 25 mcg of T3.
You can see that the numbers are shifting away from being T4-centric and giving T3 more value.
Even though this chart is still better than the original, and based on newer studies, I find that it’s may still leave a large number of patients underdosed.
Because of that, I’ve created my own conversion chart which is less conservative and based on my own experience.
My Personal Conversion Chart
I find this chart to be more useful for most people as it makes the claim that T3 is around 3x more potent than T4 and this idea is supported by studies.
These studies tested the relative effectiveness of T3 and T4 in suppressing TSH from the pituitary.
They found that T3 was slightly more than 3x more potent than T4 (3) (which is similar to the calculations below).
You can find the conversions below:
| Armour Thyroid | NP Thyroid | Synthroid (T4 only) | Cytomel (T3 only) |
|---|---|---|---|
| 30 mg | 30 mg | 37.5 mcg | 12.5mcg |
| 60 mg (1 grain) | 60 mg (1 grain) | 75 mcg | 25mcg |
| 90 mg | 90 mg | 112 mcg | 37.5mcg |
| 120 mg (2 grains) | 120 mg (2 grains) | 150 mcg | 50mcg |
You’ll notice here that I am suggesting that 25 mcg of T3 is roughly equal to about 75 mcg of T4.
That makes T3 about 3x more potent because 3 times 25 is equal to 75.
It still isn’t perfect from the perspective of NDT to T4 conversion but it’s a good starting point.
If you run the numbers on NDT you will find that this chart still underdoses you slightly when you transition from T4 to NDT.
If 1 grain of NDT contains 38 mcg of T4 and 9 mcg of T3 and if T3 is 3x more potent than T4 then 1 grain equals 65 mcg T4 equivalents (38 + (9×3)).
This 65mcg of T4 equivalents is slightly lower than the 75mcg of T4 that you may be converting from.
The difference isn’t big but it’s still there.
For these reasons, don’t use these charts as ABSOLUTE guides! They are only rough estimates to help you figure out what your body needs.
Factors That May Affect Conversion
I mentioned before that it wouldn’t be as easy as just plugging in your current dose and then transitioning to a new dose.
Why?
Many factors impact how well your body is able to utilize thyroid hormones and which thyroid hormones you do better on.
Some factors, such as genetics, are out of your control but there are others that you should be aware of.
Unfortunately, many of you reading this probably struggle with at least a handful of these other factors because of how they interact with the thyroid.
For instance:
It’s fairly common to see people with hypothyroidism struggle with their weight.
For this reason, many hypothyroid patients undergo extensive dieting programs which can negatively influence thyroid metabolism.
This changes what type of thyroid medications you may do best on and your conversion table!
It would be impossible for me to create conversion tables based on each factor below but you should be aware that these things DO impact your thyroid function and therefore your conversion.
Here are the most common things that do this:
- Your weight (4) – The more weight you have the more thyroid hormone you are likely to need. Your thyroid controls your metabolism and the more weight you have the more energy you may need to burn. We used to dose thyroid hormone based on weight alone (some doctors still do this) for this reason.
- Recent weight gain – A recent change in your weight is going to impact how your body utilizes thyroid hormone. This will probably result in an INCREASED demand for thyroid hormone in your body.
- Recent weight loss – Recent HEALTHY weight loss will mean you need less thyroid hormone but recent UNHEALTHY weight loss may require more. I know you probably want to lose weight but you MUST do it the healthy way or you risk damaging your metabolism and thyroid.
- Inflammation – Inflammation, commonly found in thyroid patients with Hashimoto’s, can cause conversion issues (5) and may impact how much T4 or T3 you need.
- Prescription Medications – Prescription medications can block the effects of thyroid function (such as T4 to T3 conversion). Sometimes medications can positively impact your thyroid so don’t be afraid to use them but do be aware of them.
- Supplements – Supplements, especially if you use the right ones, may positively alter the type and dose of thyroid medication that you need. If you haven’t already, be sure to look at thyroid-specific supplements which may help.
Conclusion
You can get away with using any of these charts, but you should always be prepared to make adjustments to your thyroid medication based on your lab tests.
As long as you don’t assume that the chart will be enough and it will get you where you need to go you will do well.
I find the best results with my own personal chart but feel free to use the one that suits your philosophy and personal preferences.
Now I want to hear from you:
Are you thinking about converting between thyroid medications?
Have you tried to convert between thyroid medications?
If so, how did your conversion go?
Did you notice a rise in your TSH? A drop in your T4 or T3?
If you used any of these tables, or something else, please comment and share what worked for you!
Scientific References
#1. https://www.ncbi.nlm.nih.gov/pubmed/24673558
#2. https://academic.oup.com/jcem/article/98/5/1982/2536971
#3. https://www.ncbi.nlm.nih.gov/pubmed/402379
#4. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3821486/
#5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3978663/





