- Synthroid is an inactive T4 that requires conversion to active T3 in your tissues. If you have inflammation, gut issues, genetics that limit conversion enzymes, or endocrine-disrupting chemical exposure, this conversion fails and you remain hypothyroid despite normal labs.
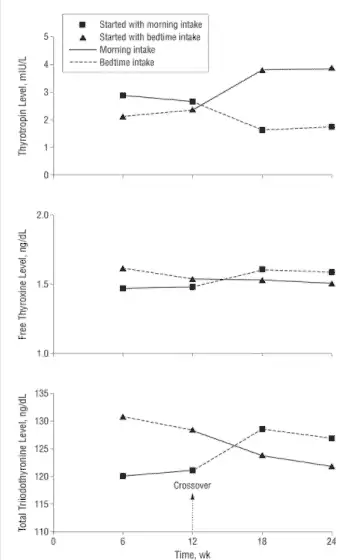
- Take Synthroid in the evening on an empty stomach to maximize absorption and serum stability. Morning dosing is faster through your GI tract; evening dosing allows more time for absorption and produces higher free T3 and free T4 levels.
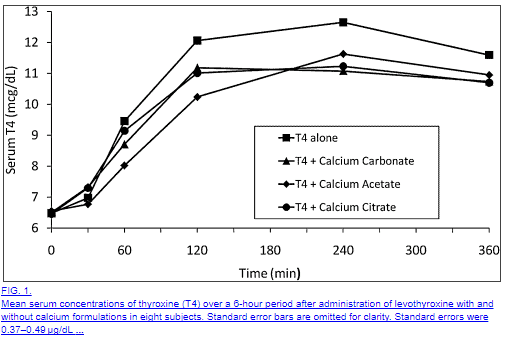
- Never take Synthroid within 4 hours of iron, calcium, or antacids as they block absorption completely. Many patients take their medication correctly but absorb only 60-80% of their dose due to medication interactions they don't know about.
- About 15% of hypothyroid patients don't convert T4 adequately and need T3 medication added to their regimen. If you've been on Synthroid with persistent symptoms and normal TSH, you likely need T3 in the form of Cytomel, liothyronine, or NDT.
- Monitor free T3, free T4, and reverse T3 levels, not just TSH, to know if Synthroid is actually working. TSH can be normal while your tissues remain hypothyroid if reverse T3 is high or free T3 is low.
Synthroid is a T4-only thyroid medication used to treat hypothyroidism.
It’s not as commonly prescribed as levothyroxine (which is its generic version) but there are a lot of patients out there using this medication.
But just because it’s commonly prescribed doesn’t mean it’s the best option or that it’s without faults.
If you’re taking Synthroid, here are 10 things that you should know:
#1. Synthroid Is Inactive
As a thyroid medication, Synthroid comes in an inactive form.
Yes, your body can activate it, but that requires a few extra steps, and not everyone does this equally well.
This activation process is referred to as thyroid conversion and it’s a big stumbling block for many people taking T4-only thyroid medications like Synthroid and levothyroxine.
What does this mean for you?
It may be entirely possible that you are taking Synthroid faithfully and it is being actively absorbed in your body BUT it is not being activated in your tissues.
")
This process may lead to persistent symptoms of hypothyroidism despite having normal thyroid lab tests and a normal TSH.
So what causes peripheral thyroid conversion issues?
Well, glad you asked!
It’s actually an evolving topic but we know for sure that these factors may contribute:
- Genetics – Sometimes genetics work for you and other times they work against you. It turns out that some people have mutations in the enzyme responsible for the conversion of T4 to T3 which make it work less efficiently. Individuals with this genetic mutation, known as a SNP, will not convert T4 to T3 as well as other individuals. Currently, the testing for this SNP is not standardized but you can make educated guesswork based on thyroid labs.
- Medications – It is well known that certain prescription medications may interfere with thyroid conversion. Medications such as anti-hypertensives, diabetic medications, and seizure medications are all included in this list. If at all possible it may be worth a look at your medication list to determine if you can consolidate medications or even change medications to see if it improves thyroid function.
- Inflammation – Systemic inflammation from any cause may reduce T4 to T3 conversion in the peripheral tissues. You can assess for systemic inflammation with serum markers such as ESR, CRP, and ferritin.
- Intestinal issues – A large portion of circulating T4 is actually converted into T3 in your intestinal tract known as the “gut”. Therefore it makes sense that certain intestinal diseases may limit this process. If you suspect peripheral thyroid conversion issues you should evaluate for conditions such as acid reflux, intestinal dysbiosis, SIBO, IBD, and IBS.
- Endocrine disruptors (the environment) – Endocrine disruptors are chemicals that humans come into contact with on a daily basis and are found in plastics and other manufactured products. Small amounts of these chemicals don’t seem to cause a problem for most people but certain individuals (probably due to genetics) may be particularly sensitive to them. Furthermore, studies from the endocrine society have shown that these chemicals alter serum thyroid lab markers and may make interpretation of these tests difficult.
#2. Synthroid Will Only Work If It’s Absorbed
Another important consideration is the topic of absorption.
Meaning: are you actually absorbing the medication that you are taking?
It sounds silly, and many people just assume that they are absorbing their medication without a problem but that may not necessarily be true.
Do you remember what the pharmacist tells you when you pick up your medication?
They probably remind you to take your medication on an empty stomach or first thing in the morning (this is fairly standard).
They want you to take your medication on an empty stomach because that gives your body the best possible chance of absorbing as much medication as possible.
Taking Synthroid with food, medications, supplements, and juices/drinks/coffee may impair intestinal absorption of your medication.
Why is this important?
Because if you are taking 100mcg of Synthroid you want to make sure that that 100mcg makes it into your body.
If you take it with food then you might only be getting 80mcg of the 100mcg dose.
Here is a list of medications that are known to reduce Synthroid absorption (5):
- Iron Salts
- Calcium carbonate (6)
- Sucralfate
- Aluminum-containing antacids
- Raloxifene
- Chromium picolinate
- Sevelamer
- Colesevelam
- Lanthanum carbonate
These medications include only those medications that limit thyroid ABSORPTION but remember that there are others that interfere with thyroid conversion as well.
You may have noticed that this list includes very common medications such as those that contain iron (often used to treat anemia), calcium (often used to treat osteoporosis), and antacids (often used to treat acid reflux).
If you are taking Synthroid, make sure that you are taking it away from medications that may limit its absorption!
You can avoid these pitfalls by making sure that you take your thyroid medication in a “fasted state” which has been shown to ensure more stable TSH and serum thyroid markers (7).
#3. Are Supplements Rendering Synthroid Ineffective?
Certain supplements can impair the absorption of thyroid hormones.
While other supplements may actually improve thyroid function.
Guidelines to stick to if you use supplements with Synthroid:
- If you need to take iron or calcium make sure that you allow at least 4 hours after you take these supplements before you take Synthroid.
- Iodine can help (or hurt) thyroid function – only use what is appropriate for your body and based on your natural intake of iodine from food sources.
- Take no more than 5-7 supplements in total each day.
- The combination of selenium and zinc may help improve peripheral thyroid conversion in individuals who are deficient in these minerals, you can read more here.
#4. The Time Of Day That You Take Synthroid Matters
Don’t get frustrated with me here because I’m about to say something that may run contrary to what you know about taking your thyroid medication…
And that is this:
Sometimes it’s better to take your medication in the evening as opposed to taking it in the morning.
But didn’t I just say that you needed to take your medication in the morning on an empty stomach to increase absorption?
Yes and that is still true, but this new information is also true, just for different reasons.

The idea behind taking your medication first thing in the morning is to help increase absorption because you will be in a fasted state – meaning you won’t have food to compete with the absorption of food in your stomach.
But there is one problem with this idea and it has to do with the speed of your intestinal tract in the morning vs in the evening.
Your intestinal tract is actually more active in the morning, meaning it is faster, and therefore your medication (and food) will spend less time in the small intestines where it is absorbed.
And this should make sense especially when you consider that most individuals have their bowel movements in the morning, this is because of the speed of the GI tract.
So what’s different about the evening?
In the evening your GI tract slows down which means that Synthroid, and other medications, will spend more time in your intestines which may, therefore, increase absorption.
And studies have actually shown this to largely be true as well.
One study (which tested levothyroxine) showed (8) that taking thyroid medication in the evening significantly improved thyroid hormone levels of both free T3 and free T4 and showed a drop in TSH (labeled as Thyrotropin).
And another study showed (9) that taking thyroid medication in the evening is at least as efficacious as taking it in the morning and may actually increase quality of life metrics in certain patients.
The moral of the story?
There really isn’t a downside to switching up the time of day that you take your thyroid medication but on the flip side, you might actually realize some serious benefits.
#5. How Synthroid Compares to Levothyroxine
The most commonly prescribed formulations of thyroid medication include the brand name Synthroid and the generic version levothyroxine.
For the purposes of the FDA, these medications are considered bioequivalent (10), meaning they should behave and act the same regardless of which type you are currently taking.
Both medications contain the active ingredient Thyroxine but they differ in the types and amounts of inert or inactive ingredients.
These inactive ingredients include various fillers, binders, and even color dyes to change the appearance of the medication.
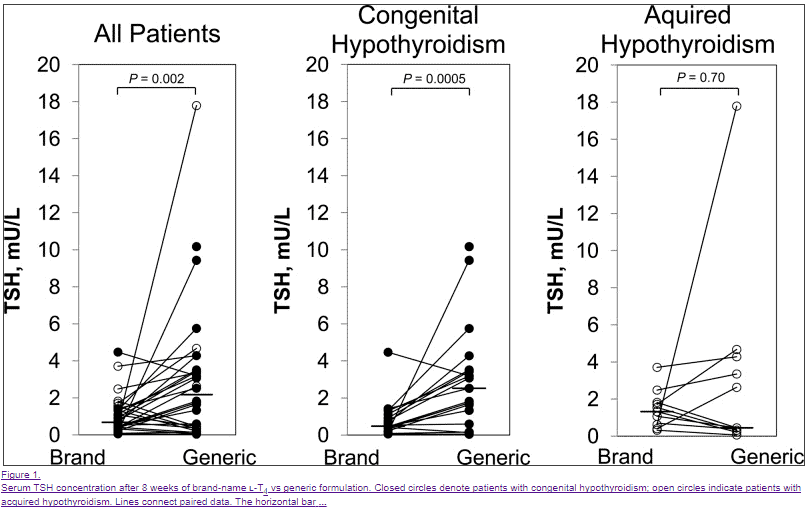
What’s important here is that these inactive fillers, dyes, and binders may actually alter the absorption and serum stability of T4 and TSH (11).
Several studies have indeed shown that Synthroid and levothyroxine are not bioequivalent (12), but this difference tends to only show in very sensitive patients such as patients who have very little thyroid reserve (those without a thyroid or with complete thyroid gland damage from Hashimoto’s).
So why does this matter?
First:
This is very important because in the United States, your pharmacist can substitute Synthroid for levothyroxine which may cause issues for some patients.
So what can you do?
If you are taking Synthroid, (and it isn’t working for you) you can request that your physician prescribe levothyroxine and put on the prescription “dispense as written” which will force the pharmacy to fill the correct medication.
This is usually only an issue for patients who are prescribed Synthroid because the pharmacy may try to save money on insurance by altering the prescription to the generic levothyroxine version.
Second:
Simply switching from Synthroid to levothyroxine or levothyroxine so Synthroid may actually provide more stable serum thyroid levels in your body and therefore reduce your symptoms.
This is worth considering for certain individuals who may be sensitive to the differences in the inactive ingredients of these medications.
#6. There Are Cleaner Options Available That May Work Better
Sometimes it’s just nice to have options when it comes to medications.
We’ve discussed that some people may do better when switching from Synthroid to levothyroxine or vice versa, but there may actually be a better option and that’s Tirosint.
Tirosint is unique among T4-only thyroid medications in that it only has 4 ingredients.
3 inactive ingredients (Gelatin, Glycerin, and Water) and 1 active ingredient (Thyroxine).
Compare this Synthroid which has a lot more (I’m not counting but you can see the chart below):

What does this mean for you?
It means that certain individuals with known conditions may benefit from the use of Tirosint over traditional medications such as levothyroxine and Synthroid.
This list includes patients who may fall into the following categories:
- Patients with gastrointestinal issues such as acid reflux, low stomach acid, IBS, IBD, SIBO/SIFO
- Patients who have experienced unexplained symptoms while taking Synthroid/levothyroxine such as rash, headache, or an upset stomach
- Patients who have not experienced significant symptomatic resolution while taking Synthroid
- Patients with decreased intestinal motility or gastroparesis
- Patients with known sensitivities to multiple medications, foods, etc.
If you fall into the categories listed above then switching from Synthroid to Tirosint may be worth exploring with your current physician.
You can also read more about Tirosint in this guide.
#7. Synthroid Only Works If You Take Enough
This is a debated topic but it’s worth mentioning here so that you are informed from the perspective of the patient.
As you’ve probably noticed your dose of thyroid medication is usually determined by your serum value of TSH.
But what is TSH?
TSH stands for thyroid stimulating hormone and it is secreted by your pituitary gland.
The function of TSH is to act on thyroid glandular tissue and stimulate the release of T4 and T3 thyroid hormones.
When you aren’t taking thyroid medication you can use the TSH to diagnose hypothyroidism.
If you aren’t producing enough thyroid hormone from your thyroid gland (either from conditions like Hashimoto’s thyroiditis, some nutrient deficiency, or because you don’t have one) your TSH will start to increase or elevate.
When your TSH reaches a certain point, usually around 5-10 mIU/L, you are diagnosed with hypothyroidism and your TSH is said to be too high.
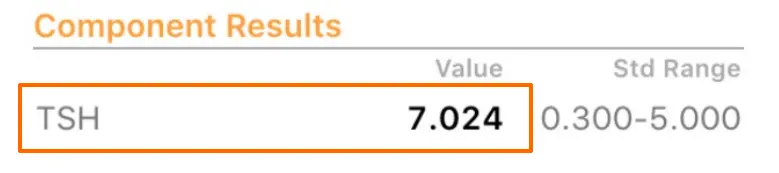
At this point, you are usually placed on thyroid medication such as Synthroid which will cause your TSH to drop or lower.
Your dose is then adjusted until you reach some TSH that your physician feels is “optimal” for you and based on other factors such as your symptoms.
This all sounds great in theory but the problem comes when we try to outline what is an “optimal” TSH level.
Most physicians tend to believe that a TSH of less than 5.0 mIU/L is probably sufficient, while newer studies indicate that a more healthy TSH is probably less than 2.0 to 2.5 mIU/L (13).
Things get even more complicated when you consider that a healthy TSH may actually be closer to 1.0 when you remove confounding variables such as the presence of Hashimoto’s in the data sample when these numbers were being determined.
The moral of the story is this:
If you are taking Synthroid and your TSH is not close to 1.0 to 2.0 mIU/L, it may be that you are underdosed or not taking a sufficient amount for your body.
While the TSH may be helpful, it’s certainly not the only thyroid lab test that you should be ordering or that can help you determine your dose (but more on that below).
#8. You May Do Better On Other Thyroid Medications
Sometimes you have to know when enough is enough.
And what I mean by that is sometimes it doesn’t make sense to stay on Synthroid or levothyroxine if it simply isn’t working for your body.
Many patients find themselves in a situation where they are continually adjusting their Synthroid dose based on their TSH but they never actually feel better.
It’s like playing a never-ending game of whack-a-mole but without some prize at the end.
So let’s be straightforward here:
Some patients will simply not do well on T4-only thyroid medications such as Synthroid.
In these patients (roughly estimated to be around 15% of all patients with hypothyroidism (14)) thyroid conversion may be blunted in a situation that results in low free T3 and total T3 levels.
It’s not exactly clear why this occurs in this subset of people but it is likely related to genetic factors and the efficiency of a very important enzyme family known as deiodinases.
What is known (at least subjectively) is that treating these patients with medications that contain T3 tends to result in dramatic symptomatic improvement.
These patients often experience more weight loss (15), a better quality of life, less depression, and higher serum T3 levels in the blood.
Medications that contain the active thyroid hormone T3 include liothyronine, Cytomel, and formulations of Natural Desiccated Thyroid.
These medications can easily (relatively) be added to your existing dose of thyroid medication and can be taken concurrently with Synthroid.
And to put this into perspective that means roughly 1 out of every 6 to 7 people will need T3 in some form added to their regimen.
If you consider that the US population is around 325 million people of which about 10% have hypothyroidism that means around 32.5 million people suffer from this disease.
If you take 15% of that number (the number of patients who have thyroid conversion issues) it’s around 4.875 million people who may need T3 medication.
That’s quite a bit!
#9. Get These Tests To Make Sure Synthroid is Working
It should come as no surprise that you need more than just a TSH to evaluate thyroid function in your body.
The TSH falls short as a universal marker of thyroid function in the body because it lacks the same deiodinases that exist in other peripheral tissues (16).
This means that the sensitivity of the pituitary gland (and therefore serum TSH levels) is different from those of other tissues making it a poor marker of thyroid saturation in distant tissues.
It also says relatively little about the peripheral conversion status of the individual or their genetics.
What does this mean for you?
It means that in order to have a more complete picture of what is happening in your body you will need more than just the “standard” TSH and free T4.
It doesn’t mean that the TSH is useless, not by a long shot.
The TSH can be still used as a sensitive marker for the identification of hypothyroidism initially, but it shouldn’t be used as the sole marker in thyroid hormone management.
Instead, you will get a more clear picture if you use the following tests:
- Total T3 – The total T3 is a marker of T3 in the body that is bound and represents a larger fraction than the free T3 portion.
- Free T3 – The smaller but more readily and biologically active form of T3 in the bloodstream.
- Free T4 – A reservoir for T3 conversion in the serum.
- Reverse T3 – An antithyroid metabolite that competes with T3 for cellular binding.
Common patterns of thyroid lab tests in individuals:
- High TSH while taking Synthroid – This is generally a sign that your dose is too low.
- Low TSH while taking Synthroid – This is generally a sign that your dose of Synthroid is too high.
- Normal TSH while taking Synthroid but with symptoms such as hair loss, cold intolerance, and constipation – This may be an early indication of poor peripheral thyroid conversion but more testing is required to determine this.
- Normal TSH with weight gain – You may be suffering from thyroid conversion issues or another hormone imbalance such as leptin resistance or insulin resistance.
- Normal TSH, normal free T4 with Low free T3, and low total T3 – This pattern may be indicative of poor thyroid conversion of low T3 syndrome.
- Normal lab studies but with elevated reverse T3 – Early thyroid dysfunction that is often seen in patients who have recently undergone calorie-restricted diets such as the HCG diet. Patients also under extreme stress will also show this profile (emotional, physical, or psychological stress).
If you are taking Synthroid, make sure you get a full lab panel to ensure you are properly analyzing your results.
Failure to check something like Total T3 or free T3 may leave you confused and confound existing lab tests and symptoms.
#10. Did You Know About These Side Effects?
Whenever you take Synthroid (or any medication for that matter) it’s always important to understand the side effects of that medication.
Hormones are always difficult to dose because the reason you are taking a hormone is that you are deficient in some specific hormone.
The problem is that the deficiency of the hormone causes side effects but the medication (or hormone) that you take to fix the problem also causes side effects.
So you may be left in a situation wondering if your side effects are from the deficiency or from the hormone you are taking to treat the deficiency!
This can get tricky, depending on the hormone, and this concept holds true for Synthroid.
Synthroid has some very troubling side effects which may mimic the side effects of hypothyroidism.
For instance:
Synthroid is known to cause hair loss by itself and hypothyroidism is also known to cause hair loss.
So what happens if you experience hair loss while taking Synthroid?
You have to figure out if it’s because of the Synthroid or your thyroid or both (You can learn more about how to treat hair loss in this guide)!
Sometimes the answer is simply taking more Synthroid and other times the answer is to stop taking Synthroid – you have to tease it out.
With this in mind I’ve put together a list of common side effects associated with Synthroid:
- Weight Gain – May be directly related to dose or thyroid conversion issues in certain individuals (read more about how levothyroxine may cause weight gain in certain individuals)
- Hair loss – Hair loss can be directly caused by thyroid medication or it can be the result of insufficient thyroid hormone (making it difficult to diagnose)
- Heart palpitations – Usually dose-dependent and related to too much thyroid medication
- Rashes – Usually the result of reactions to inactive fillers or dyes, may subside over time or when switching to “cleaner” formulations such as Tirosint
- Headaches – Usually be dose-dependent
- Insomnia – Usually be dose-dependent
- Hot flashes – Dose-dependent and usually an indication that your dose is too high
- Changes in the menstrual cycle – Usually part of the normal adaptive response as your body normalizes (usually subsides within a few months)
Remember:
You need to always consider the beneficial side effects as well as the unwanted (negative) side effects associated with any medication or hormone that you take.
Final Thoughts
Synthroid is one of many thyroid hormone replacement medications that exist.
While it may work for many people, there are many people who may require different medications and different combinations of T4/T3.
If you are taking Synthroid, make sure that you at least consider the 10 tips discussed in this article as they may be able to help you feel better.
Simply switching the type of T4 medication you are on or altering the time of day that you take your medication may be able to improve your thyroid status.
And now I want to hear from you:
Are you taking Synthroid?
Is it currently working for you?
Do you think you may need to switch or alter your thyroid medication to feel better?
Leave your comments below!
Scientific References
#1. https://doaj.org/article/94f813cafce84ed8b3558f063ef6604c
#2. https://www.ncbi.nlm.nih.gov/pubmed/28632526
#3. http://www.jscimedcentral.com/Endocrinology/endocrinology-2-1055.pdf
#4. https://www.restartmed.com/hypothyroidism/
#5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3092723/#B12
#6. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3092723/
#7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2758731/
#8. https://www.ncbi.nlm.nih.gov/pubmed/21149757
#9. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3139142/
#10. https://www.ncbi.nlm.nih.gov/pubmed/9103344
#11. https://www.ncbi.nlm.nih.gov/pubmed/9103344
#12. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3565118/
#13. https://www.ncbi.nlm.nih.gov/pubmed/19941233
#14. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5772692/
#15. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3205882/
#16. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1578599/
#17. https://www.ncbi.nlm.nih.gov/pubmed/8903695
#18. https://www.ncbi.nlm.nih.gov/pubmed/7340700
#19. https://www.ncbi.nlm.nih.gov/pubmed/19961039







I had thyroid surgery removal in May 2015, My endocrinologist surgeon put me on levothyroxine 0.15 mg . My primary care doctor took me off a month before my 6 month check up and stated it was because my levels are very high . How is that if my thyroid was remove .Had my levels checked with endocrinologist and a CT scan to make sure no tissue was still there . CT scan negative Levels still high . Primary care doctor say stay off meds six months , I have nausea light head falling to sleep weight gain . I thought it was important to keep on this meds ? Can’t get a straight answer.
Hey Artavie,
Thanks for reaching out. It’s hard to say what exactly is going on without knowing more of your history but in general when your thyroid is removed you are reliant upon taking medication to replace those levels. Only under rare circumstances can your body produce T3 and T4 without a thyroid, though it can happen. If this is the case it certainly requires further work up. Alternatively it may be possible that only a fraction of your thyroid was removed during the surgery which I have seen before as well. Your symptoms after going off of the medication are in keeping with being in a hypothyroid state.
I have been on Levothyroxine for around 35 years, I sleep a solid 8 hours every night but still wake up feeling fatigued. I have mentioned this to my Dr over the years but all my results, T3 and T4 are in the ‘normal’ range so I don’t push it any further. I was never overweight prior to this but since being diagnosed many years ago I have struggled with my weight, I walk everyday and eat a reasonably balanced diet, lots of fruit and vegies.
Hey Jewal,
There is a huge difference between being in the “normal” range and being in the “optimal” range. I find that many people feel better at higher levels of the “normal” range. I would also make sure you evaluate your reverse T3 levels and thyroid antibodies if you haven’t already.
Dr. Childs
I had a complete thyroidectomy august 2011. And was then told to take 100 mcg of synthroid. 2014 I had to have a ultra sound on parathyroid glands and it was stated I still had the most of my thyroid. I still have symptoms of hypothyroidism. I wonder why I still take the meds. I am tired nails break off and constipation is starting again.I don’t know if I should stop taking the meds or up the dosage. Right now I take 137 mcg og synthroid. What should I do?
Hey Beverly,
Thanks for the comment. It sounds like you are definitely still experiencing signs and symptoms of hypothyroidism despite being on T4 medication! You would likely see a big improvement in changing medication to something with T3. You will have to talk to your Doctor about that, my guess is you may ultimately need to find a new Doctor who is willing to work with you.
It can be tough finding a good Doctor, so I would recommend talking to other people who are local to you to find a good one.
Dr. Childs
I was diagnosed with Hashimotos in 2000. Put on .112 synthroid. Told to always take brand instead of generic. Felt ok. Two years ago I was put on levo .150 because I was so exhausted couldn’t function. Skin very dry, hair thin & breaking, nails breaking, insomnia, depression. I gradually began swinging between hypo & hyper symptoms. Heart starts pounding, heat sensitive, anxiety. I stopped taking levo for a few days and felt better but then hypo symptoms resume. I’m 53 yr old, female.Changing pcps because I’m not being heard or treated. Current pcp says there’s no difference between brand & generic. Had to argue with him just to get blood work done. Difficult to get referrals. Recent Tsh 4.26, t4 free 1.1, t3 free 3.3. He didn’t do reverse t3. I’m taking vit d3 50,000 for deficiency. With Hashimotos is it safe to take potassium iodide? Thank you for all the info you provide, it has helped me understand my condition better & gives me hope that I can one day be better balanced or cured.
Hey Sy,
Taking iodine depends on the person. In general I feel that it is usually safe to take as long as you are taking it with Selenium. I have definitely triggered antibodies in a handful of patients by putting them on iodine though, so I would proceed with caution. Start low and go slow, and make sure to take it with selenium.
With a TSH in the 4’s I can already tell that you are being under treated. In my clinic a TSH > 2.0 is an issue by itself regardless of what the other labs show and I will treat it.
Let me know if you have any further questions!
Hi Dr. Childs,
I am just beginning this journey of figuring all of this out. I am 53 years old, post menapausal. I have been on Levothyroxine for 7-8 years. Originally 50mcg, now 75mcg. I have not officially been diagnosed with Hashimotos yet, ENT said he “suspects” it. Originally, I was just told my thyroid was low and I needed medication. My most recent labs were drawn in October of 2015. My TSH was 3.68, Free T4 was 1.25. I have never had any other thyroid testing or mineral tests completed. I had a benign parotid gland tumor removed in 12/2014. I am followed by an ENT for this, 3/2015 had a biopsy for thyroid nodule, results no cancer. He ordered another ultasound of thyroid for March. I have been very exhausted for 3-4 years. I have horrible sleep, fall asleep easily but don’t stay asleep for more that 45 minutes to two hours. This has been ongoing for a couple of years. When I wake up, it takes about 1-2 hours to fall asleep again. I have NO sex drive or interest. I have been diagnosed with carpal tunnel. They recommended surgery about 3 years ago but I did not choose to have the surgery. I have pain in my feet constantly. My ankles are very puffy. I have slowly gained a lot of weight over the past 10 years. I currently weigh 225 and am 5’2″ tall. Recently, I have been very dizzy. My head feels light headed. When I turn quickly, I feel woozy but it passes. I have had a few episodes when my heart feels like it takes a “jump” and then I think I will faint. I try to calmly take deep breaths and work through that until it passes. The ENT has made a referral to an endocrinologist after I asked for a full thyroid panel. He did not do blood work but referred me on. The appt. is in MAY! Any guidance you may have would be so helpful. I have an appt. Friday 2/19 with a new family practice doctor, a DO, because mine left. I am trying to ask for full blood work be done through her but am so not sure she is well versed in hypothyroidism. Oh, I take a mult-vitamin, 5000 units of D3, 500 B12 and 20MG of simvistatin for elevated cholesteral. I thank you so much in advance for your advice. Kelley
Hey Kelley,
Thanks for reaching out. I hope you have luck with this new doctor! When you go in I would ask for this panel: TSH, free t3, free t3, reverse t3, thyroid antibodies, sex hormone binding globulin, ferritin, iron, TIBC, vitamin B12 and Vitamin D. These tests will give you a good baseline as to what is going on.
In general I find that most patients do better on some form of T3 therapy. Most often just switching to armour thyroid or naturethroid is enough to boost energy and improve symptoms. If combined with replacing B12 deficiency and Iron, then patients usually feel significantly better over a few weeks.
Let me know if you have any other questions.
Don’t forget the CoQ10 to go with that statin.
Maybe get off the gluten & sugar.
Hi Dr.Childs,
I am a male 60 year old lining in Hamilton Canada and since we moved from Germany to Canada 15 y ago my body was getting weak and weaker until 5 yeras ago the family doctor give me the Levotroxin start with 0.75 now I am by 0,125mg
And still very weak no power fatique and not happy live.
I was very interestet in you facebook information and my prob is I don’t drin smoke and eat to much I have a healty life with fruit and Vitamine tab and Kelb selenium chrome but still very weak
Can you please help me and how can I chenge the Levotroxin my Doc told me I am healty but I know that Somthing is wrong with me.
Thanks
Hey Jamal,
It can definitely be tough living with hypothyroidism. I would recommend going to your doctor and asking if you can change medication to something that includes T3 in it. That would include medications like: armour thyroid, westhroid, naturethroid, or liothyronine. Most doctors do NOT feel comfortable giving out these kind of medications, so you may ultimately need to find a new doctor.
Great job on eating healthy and your diet! It’s such a huge part of improving your overall health and thyroid function, but depending on the cause of your hypothyroidism – it may not be enough. My goal is to always get patients off of their medication, but it just isn’t always possible. In some cases, especially if your disease is due to a thyroiditis or autoimmune disease, the thyroid gland can become permanently damaged and you may be reliant upon medication for life.
Let me know if you have any further questions!
Hi Dr.Childs,
thank you very much I sah my Doc and he give me the Liothyronine 25mcg but first I do the bluttest and after 30 days again to see the result the TSH now was 0,26 T4 20 andT3 5,2.
In Ontario is only Liothyronine averrable becuase they had problem to find it.
Thanks again.
Hey Jamal,
That’s great! Let me know how it works out for you.
Diagnosed hypothyroidism in 11/2013, level 0.8. Went from hypo to hyper then finally stabilized at 1.6, and on 100 mcg of Levo. Also history of celiac disease and fibromyalgia. In January, had my tsh redrawn, was 6.9. Currently on 112mcg Levo. My endocrinologist says I have hoshimotos, my weight gain, 60 pounds in two years, is not from my thyroid, it’s because my pain isn’t being adequately controlled. Nothing other than a tsh level has been drawn, nor has the factor of my celiac disease been taken into play, since my absorption rate is different. I eat pretty healthy and have always been able to drop weight at a drop of a hat. Now, all I’m doing is gaining weight. Low carbs, minimal sugar, no sweets, protein health drinks. Something is definitely going on if my thyroid keeps going out of whack. Any additional help would be greatly appreciated.
Thank you.
Hey Kimberly,
Chronic pain can be a symptom of tissue level hypothyroidism, so those two conditions may be linked in your body. You can read more about it here: https://www.restartmed.com/hypothyroidism-chronic-pain/
The fact that you are gaining weight despite eating in that way makes me think you may have some degree of insulin resistance or leptin resistance. Make sure you get your hormones evaluated by someone who understands hormonal balance!
Hi dr.Westin Childs
I am 60 years old female, who is in constant pain since December 2015 till now. I was diagnosed with Hypothyroid in 2000 and in 2006 my doc said it is Hashimoto disease. I was going on and off on typical Hashi symptoms being on Synthroid dose of 0.100. Now for the last over 10 weeks is a terrible time for me- pain in the left side breast, actually is around the under the nipple and exactly inside nipple, also under the arm, pain in the entire left arm, the left side chest area, light head, I faint once, dizzy, during the middle of the night the strong palpitation wakes me up and my body is in huge tremor, my head and neck is hot…I did not sleep, even if go back to sleep it last just 20-30 min and again the hard palpitation/pounding wakes me up…
I visited doctors, they refer me to mammogram and a few blood work test and also to have EKG. All test results are in range, so my doctor said I am fine but I am paranoiac ….!!!!
Dear dr. Westin is it any hope for me to go back to my daily routine, how can make my doc to look for the correct diagnose in my difficult time….amy advise… Thanks in advance for your professional comment
Hey Grace,
If you aren’t getting the right answers from your current doctor you are likely going to need to find a new one. It’s much easier to do that then try to convince a Doctor that they are wrong.
There is a chance you can get your life back, but you need some guidance to get there. Look for a doctor that specializes in functional medicine.
Thank you dr. Westin for your comment. Appreciate
Hello,
I was diagnosed with thyroid cancer in May of 2015. I had a total thyroidectomy in June and after a 2.5 hour surgery the surgeon told us that I had hashimotos, probably for years. After an iodine radiation treatment I was put on 100 mcm of the generic version of synthroid but when I didn’t feel any better after 6 months and they bumped it to 125 and changed it to name brand. In March of this year I began feeling like a completely different person! So much energy, so much happier, but within the past month or two I’ve started feeling tired again, my eyes are puffy and swollen all the time and my head feels foggy even though I’m getting plenty of sleep. I’m having bouts of depression and anxiety again. Its not everyday but it’s starting to get more frequent, even though at my last check up my dr said my numbers were normal. On days when I know I have a lot to get done I’ll take 2 pills and feel 100x better and I’m starting to wonder if it’s possible that I’m building a tolerance to the medicine? Just curious if there’s a different medicine I should try?
Hey Hannah,
Yes you might be dealing with receptor resistance.
Hello,,Dr. Childs. I’ve been having a weird problem with my synthroid that just started recently. For almost a decade I was fine with taking 175mcg of synthroid. I was able to exercise and maintain a weight of 187lb. All of a sudden, I can’t tolerate synthroid anymore. My doctor took me down from 175, to 150, and then down to 125mcg. The odd part is that my TSH wasn’t particularly low on 175mcg. It was slightly below the normal low range. At 150 I was at a 2-3 and still felt terrible. I got lowered to 125 and the symptoms got better but then I got extreme fatigue and slept all day. The symptoms I was experiencing on 150-175mxg were heat intolerance, muscle weakness, dizziness, fatigue, lowered exercise tolerance, and bloated stomach. My doctor thinks it’s just age and the older you get, you sometimes get very sensitive to synthroid. I don’t want to go hypo just to avoid feeling these terrible symptoms. Is there an alternative to synthroid that I can take? Or is the synthroid making some yet unknown condition that I may have worse?? Thank you for any advice you might be able to provide.
Hey Frank,
There are many other medications you can look into. In general I find that men do better on T3 than on T4 preparations, especially if they have insulin resistance.
Dr Child’s -I was likely hypothyroid for years before diagnosis but I had no symptoms just a Tsh of 3.3 but I felt great! Two years later my Tsh was 6 and I was having heavy menstruation and constipation. I was started on Levo and I felt bad and started loosing my hair and my constipation and periods never got better no matter the dose. My t3 stayed low so I tried ndt and I felt even worse more hairloss thyroid felt swollen, I tried synthetic t3 and t4 and that’s the best I did but still not good again. I added mag and my periods and constipation resolved teo pregnancies and my symptoms were absent just to come back post Partum three months later..what can I do I have down paleo and but out foods, incorporated supplements healthy eating and rejuvenating excercise and meditation..I was better off without these meds
Since you are not accepting new patients can you recommend other doctors in the Scottsdale/Phoenix area?
Hi Judy,
Unfortunately I don’t have any recommendations to give, in order to learn this type of information Doctors will have to educate themselves so they tend to be few and far in between.
I’m on 200 mcg of Levox. I still can’t loose weight. I was wondering what supplements I could take to enhance the thyroid medicine. Thanks for your help.
Hi Brenda,
You can find more information about using supplements for your thyroid here: https://www.restartmed.com/thyroid-supplements/
And here: https://www.restartmed.com/natural-thyroid-supplements/
Dear Dr Childs
I’d love to know your thoughts on the relationship between alcohol drinking and thyroid function, especially in post menopausal women. I became hypothyroid at 58 TSH 5.9 and told my doctor I drank 2-3 glasses of red wine everyday at dinner. He never said anything derogatory even tho I suspected it to contribute to my health concerns. I wish your practice was in Maine.
Thank you
Nina
I’ve been taking Euthyrox 50ml for the past five years. I take it in the morning on an empty stomach and wait 30 minutes for my first coffee. I steel have some hypothyroid simptoms like fatigue and weight gain. I would like to switch and take the Euthirox in the evening. Can you give me the exact directions how to take it?
Hi Leora,
You can learn more about how to take thyroid medication in this guide here: https://www.restartmed.com/take-levothyroxine/
Hi.
I am 51. I am vegan. I am in exceptional shape. I had my thyroid removed in 2008. I have been on Lev. 125 since the operation. I moved changed doctors and he switched my meds. I quit him and went to another dr. Recently she switched me to 150 because I was at 6. I got another test and went way below 1. I have NO symptoms accept maybe an occasionally tingly lip. We agreed to try Synthroid 125 for a month. I am wondering about the other alternative that doesn’t have fillers and begins with a T. I am lactose intolerant and it seems as if I am not absorbing my meds. But I feel great! What do you suggest?
Hi I am sick and tired of being sick and tired. Initially treated for bi polar disorder. Amenorhea and lactating over 3 years! Then a Psych asked the question! That was over 23 years ago. I am still on that crazy medication ride of ups and downs. PCP today relies on the 2basic tests and outdated norms. I do not tolerate sugars well. I eat pretty healthy. No red meat or cow milk. Whole grains veggies & fruits. Last labs were 08/16 TSH 3.85 & free T4 1.3 dosage 125mcg Synthroid. PCP tells me I’m normal. I feel miserable. Thank you for your valued interest in we, who desperately need Drs of your caliber.
Can you tell me if these numbers look good I’m curious. Thanks in advance!
FEB 8, 2018 – Synthyroid 100mcg 6 days per week 7th day 150mcg (15mcg Cytomel). I FELT decent on this and the test below got 50mcg synthyroid removed from my Thyroid treatment.
TSH low due to thyroid cancer.
FEB 2018- Results
FT4 (0.93-1.7) ……1.32
T3 (80-200) ………108
TSH (0.27-4.20) ……0.052
MARCH 2018: Retested with FT3,FT4,TSH and ReverseT3 (results not back yet)
FT3 (2.0 – 4.4) 2.980
FT4 (0.93 – 1.7) 1.23
TSH (0.27-4.20) ……0.076 (L)
Ive been on this new dose (100mcg synthyroid ) for 6 weeks and have had so many hypoglycemic issues. I had my Sugar tested and it’s fine. Not sure if the synthroid change is doing it? Im also on 15mcg per day of Cytomel,this never changed.
I started taking Synthyroid at the 25mcg dosage. My 6-week labs showed no difference, so my dosage was increased to 50mcg. Upon increasing the dosage, I began having migraines even though I’m on a daily migraine preventative medicine. My migraine medicine was not working, and I had to visit an Urgent Care to get a shot. This occurred while on vacation. I didn’t put the migraines together with the increase in dosage until I had headaches for 9 days straight. My Dr. feels my body is just adjusting to the increased dosage, but I am feeling very worried. Isn’t 9 days enough time to adjust?
Hi Tricia,
It can take weeks for the body to adjust to thyroid medication dosing, but, that being said, it doesn’t necessarily mean you should suffer through negative side effects while it does.
Hi Dr. Childs,
I’m having an issue normalizing my TSH. I was diagnosed with Hashimotos in my late 20’s. I’m now 58 and and am breast cancer survivor that had chemo and radiation.During treatment I was on 112mcg of Levothyroxine and my TSH was very low .067 Thyroxine Free 1.35 but my anxiety was high and my Doc lowered me to 100mcg Levothyroxine and my TSH 2.035, free T4 1.05 and free T3 2.47. After being on 100 mcg. Levothyroxine for almost a year my eyelashes and hair started to fall out and my TSH – 3.49Free T4 – 1.3 and Free T3-2.2. My doctor changed my medication to Synthroid and to take 100mcg/112mcg every other day. After 1 year and 3 different doctors and many tests, I was taking 112mcg/100mcg every other day and my
TSH – .086 T4 1.5 ng/dL T3 total -77 ng/dL. Then I was put on Synthroid 100mcg and my TSH shot up to 4.84 Free T4- 1.5 HYROID PEROXIDASE AB 1 IU/mL. My doctor then told me to take 112mcg 3 times a week and 100mcg 4 times a week. Results:TSH 3.36 T4Free- 1.6 Free T3 -2.7. My Doctor then decided to alternate to one week 100/112mcg every day and one week 3 days 112mcg 4 days 100mcg: TSH-2.82 T4Free -1.5 Total T3- 84ng/dL. Did the same for another 66 weeks and my TSH went up quite significantly TSH-4.38 Free T4-1.5 T3,FREE 2.7. I am totally perplexed as to why after taking the same dos my TSH went so high. It seems as though I am not absorbing my Synthroid. It just makes no logical sense as I haven’t changed anything. All I know is that I don’t feel good and seemed to feel best when my TSH was in the lower range also my hair and eyelashes are falling out again. Do you think that Synthroid is the reason? Am I on too low a dose, or is it that I’m on the wrong type of medication. It just isn’t logical that my TSH is so sensitive ( I know that chemo and radiation shrunk my Thyroid gland). I’m very frustrated and wanted to know your thoughts.
Thanks!
Melissa
Hi Melissa,
It could be that you respond better to the generic over the brand. You can read more about why these medications are not necessarily bioequivalent in this post: https://www.restartmed.com/synthroid-vs-levothyroxine/
MSchneider@cornerstoneservices.org
Absolutely love this article! I have been a nurse for more than 20 years and this article truly helped explain the very complex thyroid in an easy to understand article. I have also suffered from severe fatigue, generalized weakness, heart palpitations and tachycardia for years and have had my thyroid tested more times than I can count but have always been told the results are normal. I would like to try a thyroid medication but not sure how to get my doctor to agree with me. Which medication would you recommend in my case? Thanks for the great information.
Hi Michelle,
I’m glad you enjoyed the article! In regards to your question, choosing the right medication can take some time and careful thought. I’ve created a resource designed to help you do just that here: https://www.restartmed.com/thyroid-doctor/
Hi Dr Childs!
Thanks for all this great information.
I had my thyroid taken out due to papillary Thyroid cancer in Feb 2018. My symptoms seemed to get a little better, but now I’m noticing they’re really quite the same as before the cancer. I was also diagnosed with Hashimoto’s in Dec 2017 right before they found the cancer.
I recently got my dr to switch me from 125mg of Synthroid (generic) to 10 mg Cytomel and 100 mg Synthroid. I started taking my Synthroid at night this week. The Cytomel is twice a day.
I’m switching drs this month because my current one will only run TSH and T4 lab panels. My symptoms include palpitations, weight gain, cold intolerance, hyperhyrdosis, constipation, brain fog, depression, difficulty falling asleep (most recently) and exhaustion. I feel like these symptoms are all over the map.. some indicating one issue, others indicating another. My T3 was tested back in May and it was in range (3.3 I think). I’m hopeful this new dr will be willing to a.) Consider other meds, and b.) Run a full thyroid panel. Any suggestions you might have are welcome. Thanks again for all the info. If there are other sources of info that youd be willing to share I’d be interested in that also.
Hi Dr. Childs,
I’m currently taking Levothyroxine (injection form). I formerly took the pills, but I am still getting the unpleasant side effects of nausea, stomach cramps,& sweating. My doctor seems to think that I have a GI problem. I dont have a GI problem. I’m just sensitive to most thyroid medications. I had the same reaction to the PILL form of synthyroid & armour thyroid. What would be a solution to resolve hypo symptoms (my TSH is too high) without all of the other yuckies? By the way, my thyroid was removed due to Grave’s disease. Thanks!
Hi Chasity,
You could try Tirosint which may help: https://www.restartmed.com/tirosint/
Hi Dr. Childs,
My wife had the iodine radiation treatment about 12 years ago. Different doctors have bounced her between Synthroid and Levo. At present, she is on 75mcg. Sometimes she will have what I would call tremors. Shaking like she was using a jackhammer. She has mood swings that make me want to hide at times. She is always cold. We live in southwest Florida. We also keep the house between 80* and 82* year round, but she still lays on the couch covered up because she is COLD. I noticed that insomnia is one of the possible side effects of Levo. She is also taking Zolpidem every night. What can she do to stop the shakes and being so cold?
Please help. Our Doctor suggested she start on a B complex
Hi Barbara,
Cold intolerance (which is what your wife is experiencing) is a symptom of hypothyroidism and an indication that she is probably not be treated appropriately with her thyroid medication. I would take a look at this article and compare her labs to those found here: https://www.restartmed.com/normal-thyroid-levels/
I am wondering if a RT3 of 23.4 (range 9.2–24.1) is considered high? What is ideal number? Also if B12 is 345 (range 187–883) is this too low? And if so, would vitamins be sufficient or are injections better?
Hi Sandra,
You can learn more about reverse T3 in these articles but the answer to your question is yes, your level is high:
https://www.restartmed.com/reverse-t3/
https://www.restartmed.com/free-t3-reverse-t3-ratio/
I like to see Vitamin B12 levels much higher, especially for thyroid patients.
You can learn more about B12 here:
https://www.restartmed.com/b12-deficiency-hypothyroid/
Hi there!My dilemma is that both on Synthroid and on Armour, from 75-88 m g Synthroid/Levo to 60 mcg Armour, my tsh and t4 are low but my free t3 is low end normal. Is this a gut/absorption issue? I am not Hashimotos. What else could be causing this…my doctors (I have tried three) are frustrated and not sure what to do with me. My November 29, 2022 labs after 60 days on Armour at 60 mcg.
Nov 29, 2022
9:14 am Thyroid Stimulating Hormone (TSH) 0.080 uIU/ml 0.358-3.740 uIU/ml L
Nov 29, 2022
9:14 am Free Thyroxine 0.61 ng/dl 0.76-1.46 ng/dl L
Nov 29, 2022
9:14 am Free Triiodothyronine 2.68 pg/ml 2.18-3.98 pg/ml
hr