- The concept of optimal thyroid lab ranges, while popular in the thyroid community, can actually cause more problems than it solves when used as the sole guide for treatment.
- Chasing specific lab numbers without considering your symptoms can lead to overmedication or unnecessary dose changes that make you feel worse.
- Every person has their own unique set point for thyroid hormones, so what is optimal for one person may not be optimal for you.
- A better approach is to use your symptoms as the primary guide and your lab tests as supporting information rather than treating the numbers alone.
- If your doctor is only adjusting your medication based on lab values without listening to how you feel, you are not getting the comprehensive thyroid care you deserve.
Among thyroid enthusiasts, there is often a big push to help people understand the difference between optimal thyroid lab tests and normal thyroid lab tests.
This way of viewing thyroid lab tests has led to improved outcomes in many patients over the years.
But there’s one big problem:
It’s not the right way to look at thyroid lab tests.
In fact, using this method is more likely to cause problems than to actually help.
In this article, I want to break down the concept of optimal lab tests and discuss why I actually don’t use this method when treating patients and why it can lead to serious problems for many patients.
What are Optimal Thyroid Lab Tests?
This may ruffle some feathers but it’s something that needs to be discussed.
If you are new to thyroid management (or the thyroid world in general) then allow me to briefly explain what I am talking about here.
There’s no question that thyroid patients, as a whole, have really been undertreated and ignored by many physicians.
I’m not discounting that fact, not by a long shot.
But the management of thyroid patients, in general, has led to a hole in their treatment.
This hole has been filled by information (some good and some bad) regarding various treatments and therapies designed to help thyroid patients feel better.
One of these alternative views has been to take a closer look at thyroid lab tests while evaluating your labs in the context of optimal levels versus simply looking at normal levels.
And this idea has been grabbed and utilized by many providers and patients, especially those people who are desperately seeking help.
Why has it become so popular?
It just makes sense. It’s intuitive and it comes as an answer to the problems that many thyroid patients face.
Perhaps the reason they are feeling so poorly is that doctors have been evaluating their lab tests incorrectly.
There’s only one problem with this idea.
It just doesn’t work.
And I’m as guilty as anyone in helping to spread this type of misinformation by not outright writing about why it’s incorrect (until now).
The reason that I’m writing this right now is to help you, as a thyroid patient, better understand the value of lab tests and how they fit into the bigger picture.
The more information that you have at your disposal the better.
What might surprise you is that most doctors (and I’m not talking about your endocrinologist or PCP here, I’m talking about doctors who focus on the thyroid and perhaps some experienced patients) realize this is the case.
They know that optimal lab tests can’t be the only answer because they have probably tried to push their levels into these ranges but didn’t feel any different.
It’s hard not to notice as a doctor that your patient isn’t feeling better despite doing what you’ve asked but if you don’t have any further information or answers then you may be stuck.
Why focusing on optimal thyroid lab tests will lead to problems
I mentioned this previously but when I look at patients to evaluate their thyroid I really don’t pay attention to “optimal” levels.
They have a time and a place (more on that below) but for the vast majority of patients who are taking thyroid medication, they can actually lead you down the wrong path instead of the right one.
And I know that many of you reading this probably hyperfocus on your lab tests and the “optimal” ranges.
I know this because I hear from you guys on a daily basis both here on my blog and on my youtube channel about your lab tests.
I know that there is a big push and focus on looking at these optimal levels.
Let me break down why optimal lab tests aren’t as helpful as you probably think:
#1. Obtaining optimal lab tests doesn’t guarantee you will feel better.
Perhaps the most important point here is that getting your lab tests into the optimal range doesn’t guarantee that you will feel any better.
And isn’t this what you want?
Don’t you want to normalize your weight, improve your energy levels, improve your hormones, re-grow your hair, and so on?
These are the symptoms of hypothyroidism and these are the very issues that you are probably suffering from.
But I’m here to tell you that getting your lab tests into these optimal ranges does not mean that these symptoms will go away.
How do I know?
From treating hundreds of patients and experimenting and observing the results.
I used to think that getting patients’ lab tests to the optimal level was the way to go and I attempted to get them there.
I used all types of medications to accomplish that goal including T4 + T3 combinations, Natural Desiccated Thyroid, T3-only meds, and so on.
But I found out very quickly that pushing around lab tests for the sake of manipulating numbers rarely ever.
This concept applies to your thyroid and it also applies to other variables and hormones (including sex hormones!).
Your dose of thyroid medication MUST be personalized and pushing your lab tests into hypothetical optimal ranges does not guarantee that it will get there.
But what about those patients who do feel better when they get into those optimal ranges? Surely there are some people who feel great having achieved these levels.
There are some but they are the exception rather than the rule.
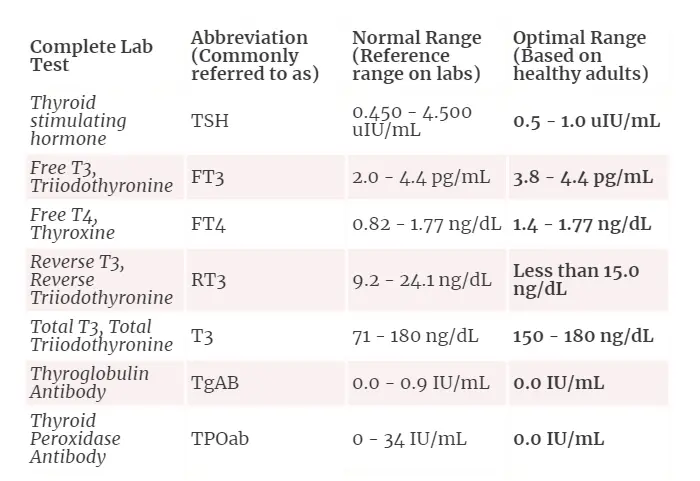
In addition, I would also submit that it’s incredibly difficult (perhaps even impossible) to obtain ALL optimal levels of thyroid lab tests for TSH, free T3, free T4, reverse T3, SHBG, and total T3 simultaneously with any type of thyroid medication.
I’ve treated a lot of people and I’ve never seen this occur.
You can push some numbers and values into the optimal range but by so doing you will affect other values and push them outside of the range you want.
It’s a teeter-totter/see-saw effect and it just leads to perpetual changes in dosing without any real impact on your symptoms.
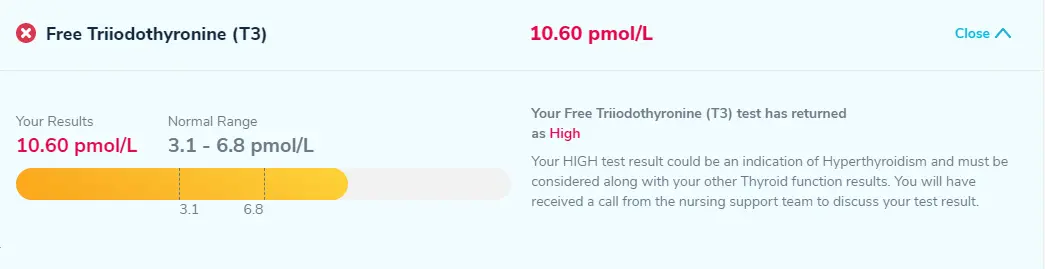
As an example to help illustrate this point you can take a look at my wife’s thyroid lab tests below:
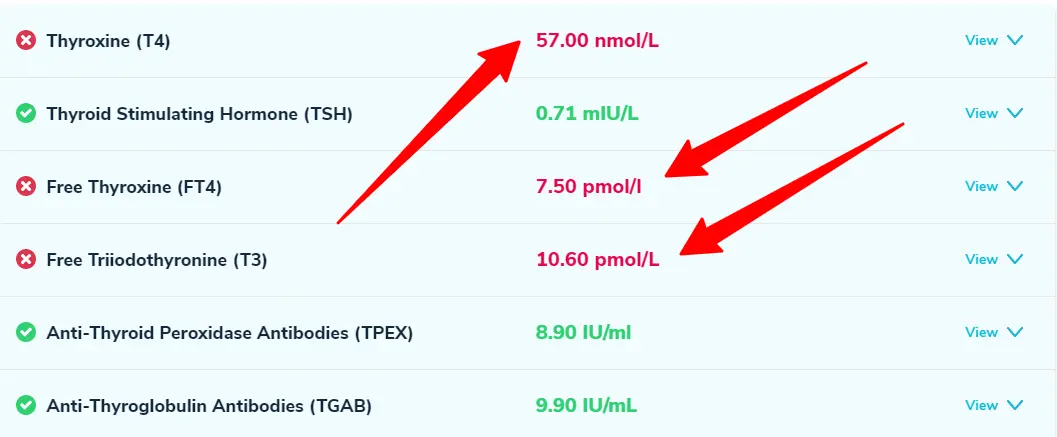
From these results you can see that her Thyroxine (T4) is low, her free T4 (free thyroxine) is low, and her free T3 is high.
These values are all outside of the optimal ranges that most people recommend and yet I consider these lab tests to be great!
She’s on pure T3 (Cytomel) and it’s sufficient to alleviate and control her hypothyroid symptoms (and her metabolism from a history of binge eating as well as treatment-resistant depression).
This brings us to our next point…
#2. If you push for optimal lab tests you may use the wrong medications.
Another big issue in focusing on optimal lab tests is that it may cause you to look at the wrong markers.
What do I mean?
What if you are someone who is hyper-focused on optimizing both your free T3 and free T4 simultaneously?
This could drive you to use a combination of T4 and T3 thyroid medications (something like a combo of levothyroxine and Cytomel) even though your body would have done better on pure T3 in a low-moderate dose.
And this is exactly the case with my wife in the example above.
She takes pure T3 (Cytomel) to control her thyroid symptoms and doesn’t need (or want) any additional T4.
But if you look at her numbers it should show that both her total T4 and free T4 are low.
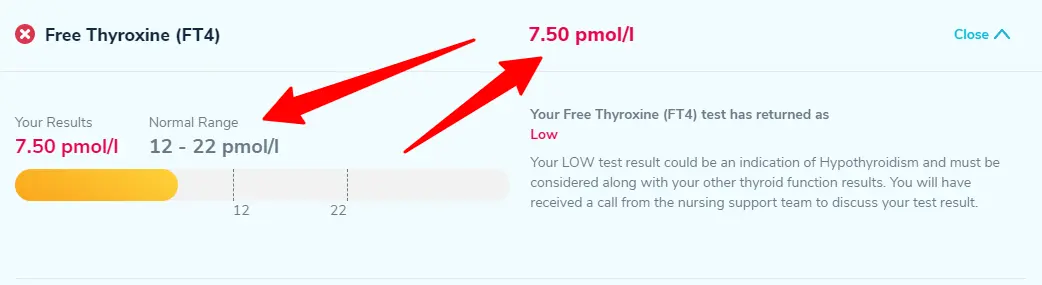
Her free T4 measures 7.5 pmol/l with a range of 12-22 pmol/l putting her significantly below the low end of the reference range.
Surely it must be bad if one of her thyroid lab tests is low? Right?
Not at all.
Remember:
T3 is the active thyroid hormone and does the job you are looking for.
In some cases, though not all, it’s fine to sacrifice T4 in order to improve T3.
And I can tell you that this is the therapy that fixed my wife’s depression and improved her metabolism after an eating disorder after many other combinations of thyroid medication/doses failed.
But you wouldn’t necessarily know this if you followed the optimal thyroid lab ranges which some people suggest must be optimized in order for you to feel good.
In fact, I’ve seen a number of people who needlessly add T4 to their existing T4 + T3 regimens to try and improve their T4!
But this typically just causes an increase in reverse T3 which is the exact opposite of what you want.
Focusing on these optimal ranges may lead you away from the very medication that could be helping you (and this probably doesn’t occur infrequently).
#3. You can manipulate your lab tests and results however you want.
Another thing you should be aware of is just how easy it is to manipulate your own thyroid lab tests.
Your thyroid levels fluctuate throughout the day on their own (1) and they rapidly change with the use of any type of thyroid medication (2).
You can actually alter how you take your thyroid medication to basically create the lab tests that you want (I don’t recommend this but it is possible).
Do you want your free T4 to be low and your TSH to be high? Simply avoid taking your thyroid medication for 3-4 days before you are scheduled to get your labs drawn.
Do you want your free T4 to be high and your TSH to be low? Simply take 2-3x your dose of thyroid medication 4-5 hours before you are scheduled to get your labs drawn (Obviously, I am not recommending you do this but I am suggesting how easy it would be to do – so, please don’t do this!).
Do you want your free T3 to be high? Simply take a little bit of extra T3 2-3 hours before your thyroid lab tests and you’ll see it jump up (see my wife’s free T3 as an example – in this case, she took her T3 medication and then had her labs drawn about 2-3 hours later).
Again, I’m not recommending you do this but you can see how changing when you take your thyroid medication can dramatically affect your thyroid lab tests.
In fact, she could have easily tripled her dose (without experiencing significant negative side effects) to make her lab tests look hyperthyroid.
The point is, while we all (doctors and patients) know that it’s easy to manipulate lab tests with minor changes in medication dosages, we don’t really know how to account for this when interpreting lab tests.
What this means is that you will see a number of different reactions to the same lab tests (especially those above) ranging from “she’s hyperthyroid and needs to stop all medications!” to “let’s add T4 to her regimen to improve her T4 levels!” and everything in between.
There are some basic recommendations on how to take thyroid medication in relation to when you get tested (such as avoiding your medication for 24 hours, etc.), and while these are recommendations that most people/doctors use they have never been proven to be the best way to look at thyroid lab tests.
It’s hard to take all of your lab tests seriously knowing how easy it is to affect your results.
Imagine making treatment decisions on false data because of lab error or error relating to when/how the labs were drawn or when/how the patient’s medication was taken.
This can and does lead to poor treatment decisions.
#4. You may be focusing on the wrong metric.
While your thyroid lab tests are an important aspect of understanding your thyroid function they are certainly not the only factor you should be looking at.
Probably more important than your lab tests (and whether or not they are “optimal”) is whether or not you feel better taking your medication.
How you feel is known as your clinical presentation or how you are feeling or your symptoms.
These are all words and phrases that describe the same thing and answer the question of whether or not you are on the right track.
It’s possible for you to have very “whacky” thyroid lab tests but still feel great.
It’s also possible for some of your thyroid lab tests to be “optimal” but for you to feel poorly.
When both of these statements can be true we have to go back and evaluate what it is that we are looking for with thyroid treatment.
What we really want is for you to feel better and not experience any negative side effects from the treatment associated with getting you there.
Where your thyroid lab tests end up, provided they don’t lead to harm, doesn’t really matter to us as long as you get your life back and can manage your symptoms.
")
The problem with focusing on obtaining optimal thyroid lab tests is that this can lead you to forget or neglect how important your symptoms are.
I’ve seen a number of people who are so focused on their lab tests that they don’t understand why they used to feel better with “low T4” or “low T3” before they changed/upped their medication.
If you solely focus on your lab tests and what your results are then you miss the chance that you could be heading in the right direction in regards to your treatment but completely miss it or change course without proper cause/reason.
Because, really, we don’t even know what “optimal” thyroid lab tests are.
We and I’m included here, just make the assumption that higher lab tests and ranges are probably a more accurate representation of what “healthy” is.
But no one has ever proven this, it’s just based on intuition.
#5. It’s not always possible to actually obtain optimal free T4 and free T3 levels at the same time.
I alluded to this above, but it’s oftentimes not even possible to obtain optimal free T3 and free T4 levels while obtaining an optimal TSH.
Why does this occur?
It has to do with how T3 medications impact your TSH and free T4.
The higher your dose of T3 the lower both your TSH and your free T4 will go.
I’ve seen people who fall into this trap and then start to add T4 back to their regimen (of whatever they are taking) to try and push the T4 back up.
But this only drives the TSH down further and leads to statements such as “the TSH is not important” or “the TSH will always be suppressed when taking NDT or T3”.
But that just isn’t true (again, see my wife’s example above).
It’s only true if you falsely believe that 1) all lab tests MUST be optimized and 2) that T4 somehow provides benefits to the body that you can’t get with T3.
The stance that TSH doesn’t matter is a poor one to take because there are some documented consequences to suppressing TSH long-term (3) in certain people.
Suppressing your TSH doesn’t guarantee that you will have negative consequences but it does increase your risk.
You can’t just wave away that data because you don’t like it and because you think that your T4 and T3 take precedence over the TSH.
I would recommend exercising caution against this type of thinking and never completely disregarding any thyroid lab test just because it doesn’t fit your current understanding of thyroid function.
What should you be looking at instead?
The question really becomes something like this:
If optimizing your thyroid lab tests isn’t the right way to feel better then what is?
And that question is a lot more difficult to answer and it’s part of the reason that I’ve avoided answering it for some time.
Having said that, I will attempt to give some guidelines to help you understand how I look at thyroid lab tests to figure out if a patient is on the right track:
- The TSH – Whenever possible I try to keep the TSH in the optimal range (0.5 to 1.0) but if that isn’t possible then I always try to get a non-suppressed TSH. A low (but not suppressed) TSH hasn’t been associated with negative outcomes. In addition, your TSH response to thyroid medication is valuable in helping to determine how high or low your total thyroid dose should be.
- Total T3 – I find the total T3 to be a much better long-term marker of T3 status in the body compared to free T3.
- Free T3/Reverse T3 ratio – The free T3:reverse T3 ratio can help you understand if your body has a sufficient amount of T3 available for cellular use. High levels of reverse T3 are often associated with hypothyroid symptoms but they do not guarantee it.
- Clinical presentation and symptoms – Discussed above.
- Other hormone imbalances – The presence of certain hormone imbalances (such as leptin resistance) can impact thyroid lab tests and distort “normal” ranges. Disordered leptin levels are often seen in thyroid patients due to how these hormones interact.
- Resting heart rate – Your heart rate is a good proxy for how thyroid function and is especially useful when using T3. A rapid heart rate is often the first sign of excess thyroid dosing and this can be tracked and managed easily.
- Blood pressure – Similar to the heart rate, blood pressure can help me understand if you have any existing hormone imbalances such as insulin resistance.
- Metabolism and calorie burn – Metabolism is closely associated with thyroid function (4) and is a great way to evaluate thyroid function.
- Current dietary/calorie intake – I pay close attention to how many calories patients are consuming because this value helps me understand how well the thyroid is functioning. People who have small appetites just to maintain normal weight often have thyroid disease associated with this condition.
- Energy levels – I use the subjective symptom of “energy” as a proxy marker for thyroid function. It’s fairly sensitive because energy levels tend to improve rather quickly once you are on the right type and dose of thyroid medication.
- Inflammation status – The presence (or absence) of inflammation is always important for thyroid function because it can impact how well your body is converting T4 to T3.
- Cholesterol levels – Particularly total cholesterol which is a sensitive marker for hypothyroidism (5) even in the setting of a normal TSH. If you have high cholesterol (without a known cause) AND hypothyroidism, there is a good chance that they are connected.
- How well you are converting T4 to T3 – How well you are converting T4 to T3 helps determine which thyroid medication you should be on. Those who don’t convert well tend to do better on T3 medications while those who do, do better on T4 medications.
I still look at the other thyroid lab test to see where they are at and how they respond but I don’t use them by themselves as a way to determine management.
They can and still should be tested for because they are part of the story, but you should also realize they are not the WHOLE story (and probably not even the main character).
When are the optimal thyroid lab ranges helpful?
Do these optimal thyroid ranges have a place in managing thyroid disease?
The answer is yes, but their use is limited and can be summed up with the following example:
Imagine if we lined up 100 healthy people and tested their thyroid function using all of the thyroid lab tests: TSH, free T3, free T4, reverse T3, and thyroid antibodies, and determined whether or not they had thyroid disease based on the optimal ranges found here.
What do you think we would find?
We would find that over 90% (probably closer to 99% or more) of these 100 healthy people would “fail” the test.
Why?
Because hardly anyone is walking around with ALL of their thyroid levels in the optimal ranges.
And that is perfectly normal for them.
So one big issue in using the optimal levels in thyroid management is that the results are far too strict and if used on a large scale would incorrectly diagnose many people with thyroid disease who don’t actually have thyroid disease.
Having said that, I do still think that using optimal ranges still has a ton of value in helping determine cases of hypothyroidism that are sub-clinical or do not present in the typical fashion.
In addition, I think using the optimal levels (for the purpose of diagnosis) is great for people with thyroid issues relating to metabolic damage and weight gain.
So we shouldn’t throw them away just because using them promotes an issue.
My recommendation for using these optimal levels is for ESTABLISHING a diagnosis of thyroid disease (hypothyroidism or Hashimoto’s) and not for the MANAGEMENT of existing thyroid disease (especially those taking thyroid medication).
Furthermore, we can fine-tune the requirements for a diagnosis of hypothyroidism and the management of thyroid disease like this:
- If you have 2+ thyroid lab tests that are outside of the “optimal” range AND have the presence of hypothyroid symptoms then this would be sufficient for a trial of thyroid medication.
- If you have 3+ thyroid lab tests that are outside of the “optimal” range AND have the presence of hypothyroid symptoms then it is likely that you have thyroid disease.
- If you are taking thyroid medication (of any type) then you should not use these optimal lab tests solely as a way to measure whether you are on the right type and dose of thyroid medication.
Conclusion
The bottom line?
Don’t focus solely on whether or not your thyroid lab tests are “optimal” and instead look at other factors including your metabolism, inflammation status, hormone balance, and so on.
By looking at all of these factors together, in conjunction with your clinical symptoms, you will be much better equipped to find what type and dose of thyroid medication you should be on.
Some of this information may come as a surprise but it represents my current understanding of thyroid function based on my experience.
If you are someone who has been hyper-focused on your lab tests and obtaining optimal results I would encourage you to read the information listed here as to why that may not be in your best interest.
Now I want to hear from you:
Are you currently feeling well on your thyroid medication?
If so, what type and dose of thyroid medication are you taking?
Does this information surprise you or have you suspected that the current optimal ranges have flaws?
Do you agree/disagree with the information provided here?
I’d love to hear from you! Leave your questions or comments below!
Scientific References
#1. https://www.ncbi.nlm.nih.gov/pubmed/716774
#2. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4557078/
#3. https://www.ncbi.nlm.nih.gov/pubmed/20151821
#4. https://www.ncbi.nlm.nih.gov/pubmed/30124904/
#5. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3109527/






Dr Childs,
Have you seen any interaction between Berberine and thyroid labs? As well as Berberine causing extremely high resting heart rates? (90+). I cannot seem to find any research on the topic and figured you may have some clinical data.
Many thanks as always for the excellent content!
DSharp
Hi Dsharp,
I have not seen anyone react in that way to Berberine and I’ve used it on many people. I have seen it happen with metformin, however.
Hi – I have no thyroid since 2015, been struggling with meds and feeling normal and well. I started to feel good with a higher dose of t3 with t4 (Tirosint) but my TSH was high( 21)My t3 and t4 were low normal range. Dr put me on a higher naturthroid dose now I feel awful again. Dr called after retesting my raised dose of Naturethroid and says I’m still hypo wants to raise Naturthroid dose higher. No way!! probably change Drs at this point. Dr. runs tests every month instead of listening to how I feel. I feel better with more T3 but Dr reluctant because of test results, so this blog is hitting home with me.
I desperately needed to hear this right now. As I sit here at 3am, being up for an hour with my racing heart, trying to get all the usual In to a perfect range, thinking TSH that is so far below normal doesn’t matter. Ugh.
I’ve gone through the Armour, Naturthroid and now the NP changes and after NP has recently changed, I stopped all my medication (NP and cytomel) and went on the supplement Thyrovanz. After 4 weeks, I just tested to find I have: free t3 and total t3 at the lowest part of the range, free T4 at the highest part of the range, TSH so low that it’s not even measurable and the reverse t3 im still waiting on.
I’ve been living (and dying) trying to get myself “optimal”. I’m at the very end of my rope. I feel absolutely horrible and have zero help from any knowledgeable doctor.
Can you give me direction? I have no thyroid due to cancer. I’m not overweight, I eat as close to paleo/keto as possible to the majority of the time. I make sure my D, Iron, and B’s are optimal. I’ve had adrenal’s tested and I work on getting my gut flora as best as I can.
I’ve never been able to get all my Thyroid levels to those theoretically optimal values (although i must confess, it isn’t for lack of trying). Still, using the concept of optimal levels has been helpful when I truly feel awful when value X is one point below the lower limit of normal or right on the line, and I’m told it’s not a big deal. Knowing where I more or less should be has been invaluable. After all, but how many times can one be told not to worry about it and not start to doubt their own sanity. Where I think optimal values are extremely helpful, and a major contributor to how well I feel, is knowing where my levels for B12, Vitamin D, Iron, Ferritin, etc., etc., should be.
I’ve been taking 150 mcg levothyroxine and 30 mcg liothyronine for a couple of years, and aside from more or less keeping the lab values in check, I don’t feel horrible, and certainly feel alot better, but rarely feel great. That being said however, I experiment with taking at different times of day, splitting up versus taking together, etc. That seems to have an impact, although my prescribed dose of liothyronine is higher, I mostly don’t take the second pill because I simply can’t get to it. Between spacing out meds from meals and taking other prescriptions at different intervals it just isn’t realistic, and can get to be quite stressful in fact. As an aside, I was excited to try Tirosint, at least until I found out it’s on the list of BCBS explicitly excluded meds.
Hi Melissa,
Just a note to let you know that I have BCBS as well, and with a little fight from my doctor explaining why I needed *this* drug as opposed to synthroid, they relented and are letting me use this drug and paying a good chunk of the price. It’s worth fighting for if your current drugs aren’t working for you.
I’m glad you take the time to look into this. I’m struggling to find a good endo who will listen to me. My endo only check certain labs and doesn’t do a full thyroid panel and then some. I’ve gained so much weight in the last year despite my labs being within their range not to mention feel like crap. I’m pretty sure I have insulin resistance as well. I definitely think this is a great article and maybe I can mention some of these tests to my endo.
Hi Melissa,
On Tirosint’s website there is a “Ways to Save” tab. Select that tab and there is a Tirosint Copay Savings Card that could reduce your cost, or the Tirosint Direct Program is listed under the same area that may be another option for reduced cost. My insurance is changing to BCBS on January 1st, 2020. Good luck to you:)
I have Blue Cross Blue Shield. I printed out the Tirosint copay savings card for my pharmacy & pay a flat $25 a month for my Tirosint prescription.
I’ve read dozens of your articles but still can’t seem to figure out how many hours prior to blood testing I should refrain from taking my NDT in order to have results that I can use to inform my dosage. You allude to the importance of timing but I don’t see any concrete guidance 🙁
Hi Aaron,
I’m publishing a video on that topic on my youtube channel very soon. You can check there or, alternatively, I will also post it to my blog roll as well.
Dr.Childs,
my last lab test show my TSH is 12.230 they is high they was before I was taking levothyroxine 88mg i stop taking them. I don’t like taking
proscription medical what will help low my TSH.
Thank you for your help I wish more doctors would help there patients like you do.
Hi Susan,
If you are looking for a natural way to reduce your TSH then you would want to look at these therapies: https://www.restartmed.com/natural-thyroid-remedies/
This is great information and makes so much sense. The problem is I need someone who can treat accordingly. I have been through so many doctors and I still don’t feel like I’m where i should be. Am I a little bit better? Yes, but I wish I could find someone who understood this info. I struggle with depression and all anyone wants to do is put me on anti depressants. I know it’s my thyroid.
if anyone knows of any great doctors in Phoenix please let me know.
Hi Jody,
Unfortunately, this type of information is not widely accepted as of yet. My hope is that more people will start shifting how they view thyroid lab testing and management after reading it.
Hi Jody,
Search on Integrative Medicine in your area. They most likely won’t take insurance… but are worth it!
Yes! Definitely what Stefanie said! Working with a naturopathic doctor is the only thing that has helped me with my Hashimoto’s that I’ve been struggling with for 25+ years.
I LOVE this and completely agree, we cannot box ourselves into a “one size fits all” scenario.
I do have a question about getting to an optimal dose in the sense that one should avoid staying complacent on too low of a dose as eventually the body’s natural negative feedback loop will cause a crash/deeper hypothyroid symptoms in time. If we just go by how we feel rather than labs, how do we know when to increase the dose to stay ahead of the negative feedback loop?
Thanks,
Sara
about getting optimal
I was diagnosed with Hashimotos in 1983. I have been taking Armour Thyroid 1.5gr for about 6 years. My TSH has always been consistent at about 0.5 mcIU/ml even though i have felt awful and have complained of feeling hashimoto like symptoms. When I asked for a free T3 & T4 and reverse T3 both my PCP and my endocrinologist said “not necessary” and my PCP even went so far as to ask me where I ever heard of those tests because they were quackery. I feel like I am being treated for hypothyroidism and not an autoimmune disease. My last two TSH tests 10 weeks ago were 9.2 and my Armour thyroid was increased to 2 grains a day. I feel even worse. My repeat TSH 6 weeks after increasing my Armour Thyroid was 10.9. Now that I am having worsening symptoms my medical teams answer is to send me to an ENT. Shouldn’t someone be concerned why my body is not reacting to my medication? I have seen so many doctors and they all seem to not know what they are doing. Where do I go from here to begin feeling human again.
Hi Lanie,
Unfortunately, thyroid patients are not at the top of the “concern” list to physicians. You will have to be your own advocate when it comes to managing your thyroid (which is why this website exists!).
But what if no matter what you do, your TSH stays pretty much fully suppressed? Even when my frees are on the low side, my TSH never gets above .1. Ever. I’ve tried only Cytomel, only NDT, combos, nothing really makes the TSH come up in the .5-1 range.
Hi Colleen,
It’s hard to say for sure but I always think of thyroid status as fairly dynamic and liquid. Whatever is happening right now in your body is no guarantee that it will continue into the future, especially if you are trying to lose weight, dealing with other hormone balances like leptin resistance, and so on. Some people can do fine with suppressed TSH levels but I find there’s almost always something else interfering with thyroid function causing the inability to improve thyroid function without suppressing the TSH.
Hello Dr Childs:
Great information, but as you said it can be very confusing.
I am on 75 mcg of T4 (Oroxine) and 10 mcg of Tertroxin and my levels are :
18/10/19 TSH 0.24 (0.4-4.0) Free T4 16.4 (9.0-19)
20/11/19 TSH 0.17 Free T4 16.0 Free T3 4.3
I have been on this mix for about 3 1/2 months with absolutely no improvement
My GP is thinking to reduce the Oroxine to 50 mcg because of the decreasing TSH…do yo think I am on the wrong dosis or should I go back to my old treatment with just T4.
I would appreciate your advise, so I can pass it onto my GP.
Thank you
Kindest Regards
María Leighton
Web doctor is the way to go. So many including me just don’t have access to a doctor that may know more than we do. I do the best I can with private testing, manipulating my dosage of T4, and working with vitamins to get my T3, but I still need a doctor to prescribe the T4 meds. Certainly there could be a better way!!! We all are crying HELP!!!
Hi Dr. Childs,
Thanks so much for this very informative post. I noted that you said, “In some cases, though not all, it’s fine to sacrifice T4 in order to improve T3.” Could you say more about this? In which cases is it NOT fine to sacrifice T4? I’m curious if having a low T4 (specifically) is a known contributor to any symptoms, such as hair loss or menstrual irregularities.
I have been taking T3 (Liothyronine) only for 1.5 years now and I’m generally feeling SO MUCH better on this regimen than when I was taking a combination of T4 and T3. However, my T4 is below the normal range and my TSH is suppressed. (My T3 is in the high-normal range). My doctor doesn’t seem concerned at all about the low T4 or the TSH, but my naturopath has suggested that I reduce my T3 (Liothyronine) dosage and add some T4 (Levothyroxine) in an effort to get my T4 in the normal range. She says that an imbalance of T4 and T3 is not great and that the end goal should be to have both of these in the normal range. Based on what I read in your blog post above, it sounds like this isn’t necessarily true.
Thanks in advance for sharing your thoughts on this!
~S
After the birth of my last child, I had some hormone stuff go crazy. One of the things my doctor did was take me cold turkey off my thyroid med (Armour).
I have had my TSH creep up to between 1.0 and 2.0, and my total T3 is low, but I feel fantastic. I have tons of energy. I am not back to my pre-baby weight, but I am not overweight, I never feel cold, and my skin is good. The only hypothyroid symptom I have is thinning hair, but this is not necessarily from hypothyroidism! My doctor wants me back on thyroid medication after 2 years off of it, and I do not want to do it.
I plan to get more regular with iodine, selenium, zinc, and essential oils for thyroid. But, even if my labs do not look perfect, I don’t really want a medication when I feel fine. Doesn’t that make sense?
Hi Maureen,
There are plenty of people out there with labs such as yours who feel fine so I wouldn’t worry about that. If you can manage your thyroid with natural therapies then that would be ideal.
Hi Dr. Childs,
In another article you wrote, you noted that it’s best to do a combo of t4, t3, and t2; but you note here that your wife is doing on well on t3 alone and doesn’t need t4 and t2. How can you tell when someone does or doesn’t need t4 and t2 along with t3?
In that same vein, Janie Bowethorpe at STTM has a whole page dedicated to why optimal does matter. Do you have any thoughts on her reasons given there? https://stopthethyroidmadness.com/optimal/
Thank you!
Hi RB,
It depends on the person, their symptoms, their lab tests, their priorities, their history, etc. In regards to my wife, I completely weaned her off of thyroid medication and she is no longer taking any thyroid hormone. What I mentioned above is really only a guide and, ultimately, you will need to use trial and error find the best solution for yourself.
I think optimal thyroid lab tests do matter, somewhat, but they aren’t nearly as important as people think. Take my wife as an example, I’ve shared her lab tests and they are no where near “optimal” and yet she was able to completely eliminate all of her symptoms, regrow her hair, resolve her depression, and completely normalize her metabolism with levels that are far outside of optimal ranges.
Does this article apply only when diagnosing thyroid disease or does it apply to both diagnosing and for people who do not have a thyroid due to a tt?
I forgot to ask another question that you touched on in this article, and that is the timing of labs when taking thyroid medication.
I’ve read too many articles on this topic and most conflict with each other. One article stated the only time to worry about the timing is when you take NDT such as Armour because it contains both T3 & T4. I’ve been sticking with the wait until after lab tests to take meds, I take Armour, is this still practical?
It seems from what you are saying, I could take my medication in the morning and wait 6-8 hours for labs. Is that accurate?