
- Endometriosis develops from estrogen dominance, where too much estrogen relative to progesterone causes abnormal tissue growth. Test your estrogen metabolites with 24-hour urine or DUTCH testing during your mid-luteal phase to understand exactly how your body is processing estrogen.
- Your thyroid function directly impacts estrogen balance. Hypothyroidism is often missed by standard TSH testing alone, so get comprehensive thyroid labs including free T3, free T4, reverse T3, and antibodies. Fixing thyroid problems can dramatically improve or resolve endometriosis symptoms.
- Confirm you're actually ovulating, as many women have regular periods without ovulation. Without ovulation, you lack progesterone to balance estrogen. Check basal body temperature daily (should be at least 97.8 degrees) or use LH urine tests mid-cycle to verify ovulation.
- Your diet shapes estrogen metabolism. Eat 2 cups of brassica vegetables daily (broccoli, cauliflower, kale) which contain DIM to push estrogen down protective pathways. Cut refined grains, dairy, sugar, and non-organic animal products, then replace with whole foods and healthy fats.
- Support your body's natural detoxification with targeted supplements like diindolylmethane, milk thistle, calcium D-glucarate, and magnesium to help your liver eliminate excess estrogen metabolites efficiently.
If you have endometriosis, there’s a good chance your thyroid may be part of the reason.
Most women with endometriosis are told the problem is “too much estrogen,” and that’s true.
But what they’re rarely told is why they have too much estrogen in the first place.
In many cases, it comes back to the thyroid.
When your thyroid is underactive, your liver slows down.
That slowdown impairs estrogen clearance. Estrogen builds up, progesterone gets suppressed, and you end up in a state called estrogen dominance, the hormonal environment that leads to endometriosis.
The good news: when you address the underlying cause instead of just managing symptoms, you can see real improvement in your symptoms.
Here are 10 ways to do that, starting with the most important:
1. Get a Comprehensive Thyroid Panel
This is the one doctors will skip, so make sure you don’t!
Standard thyroid testing only looks at TSH. TSH alone can look normal even when your thyroid is not functioning properly.
To get an accurate picture, you need a full panel: TSH, free T3, free T4, reverse T3, and thyroid antibodies.
Here’s what optimal looks like: TSH under 2, free T3 in the upper third of the reference range, free T4 in the upper third, reverse T3 under 15, and antibodies under 30.
Anything outside these ranges warrants a closer look, especially if you have symptoms like fatigue, weight gain, constipation, hair thinning, or irregular periods.[1]
You don’t have an estrogen problem if you have a thyroid problem. Fix the thyroid and estrogen often corrects itself.
An older doctor once taught me that giving 30-60mg of Armour thyroid to women with PMS and PMDD dramatically improved their symptoms.
Now I know exactly why: normalizing thyroid function restores estrogen clearance and progesterone balance.
It’s also worth noting that undiagnosed Hashimoto’s thyroiditis is extremely common and frequently missed with standard labs.
2. Test Your Estrogen Metabolites
Standard blood estrogen testing only measures estradiol, which fluctuates hour to hour and tells you very little about how your body is processing estrogen.
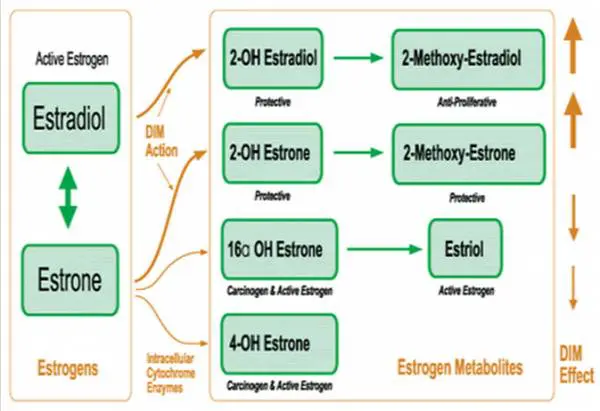
What you really need to know is where your estrogen metabolites are going: down the protective 2-OH pathway, or the more problematic 16-OH pathway.
The best way to see this is with a 24-hour urine test or DUTCH urine hormone testing. These tests measure estradiol, estrone, estriol, DHEA, testosterone, and cortisol metabolites all at once.
Test during your mid-luteal phase, around days 19-22 of a standard 28-day cycle, for the most accurate picture of your estrogen-to-progesterone ratio.
Don’t let your doctor tell you your labs are normal if they only tested for estrogen, not estrogen metabolites.
3. Check Your Basal Body Temperature
Your basal body temperature (BBT) is one of the most useful and underused tools for understanding both thyroid function and ovulation.
Check your temperature first thing in the morning, before getting out of bed.
Anything below 97.8 degrees consistently suggests low thyroid function or adrenal issues, both of which contribute to estrogen dominance.
BBT tracking also tells you whether you’re actually ovulating.
Your temperature should rise by about 1 degree after ovulation and stay elevated for around 10 days. If the rise doesn’t happen, or if your temps fluctuate wildly, you may not be ovulating, meaning your body isn’t producing the progesterone it needs to balance estrogen.
This is a direct driver of estrogen dominance and endometriosis.[5]
4. Eat to Support Estrogen Clearance
Diet has a direct impact on how your liver processes and eliminates estrogen.
The goal is to feed the detoxification pathways and avoid foods that burden the liver or add extra estrogenic load to your body.
Start by cutting out refined grains, sugar, alcohol, caffeine, artificial sweeteners, and processed foods. These increase inflammation and slow liver detoxification.
Also eliminate non-organic dairy and non-grass-fed animal protein, which often contain added hormones and antibiotics.
Then load up on brassica vegetables: broccoli, cauliflower, kale, Brussels sprouts, and cabbage, at least 2 cups daily. These contain diindolylmethane (DIM), a compound that actively pushes estrogen metabolism down the protective 2-OH anti-cancer pathway.[2]
Add omega-3-rich foods like wild salmon, sardines, and walnuts to cool inflammation, and include ground flax seed and high-fiber vegetables to support healthy estrogen excretion through the gut.
5. Exercise to Boost Estrogen Metabolism
Regular exercise improves insulin sensitivity, reduces excess body fat (which produces estrogen), and enhances liver detoxification.
Focus on high-intensity interval training (HIIT): 15 to 20 minutes, one to two times per week, to get the most hormonal benefit in the least amount of time.
This style of exercise changes gene expression, improves mood, and accelerates toxin removal.
On non-workout days, stay active with walking or movement breaks throughout the day.
Prolonged sitting slows lymphatic drainage and circulation, which can compound hormonal imbalances over time.
6. Eliminate Xenoestrogens from Your Environment
Xenoestrogens are synthetic chemicals that mimic estrogen in your body, binding to estrogen receptors and increasing your total estrogenic load, even when your actual hormone levels look normal on labs.
Common sources include bisphenol A (BPA) in hard plastics and water bottles, pesticides and herbicides on non-organic produce, hormones in conventional dairy, and even thermal paper receipts.
To reduce your exposure: eat organic when possible (especially the EWG’s Dirty Dozen), drink filtered water from glass or stainless steel containers, store food in glass instead of plastic, and avoid handling receipts.
These small changes add up significantly when applied consistently.
7. Sweat Regularly to Detoxify
Sweating is one of the most effective ways to eliminate excess estrogen metabolites and environmental toxins.
Your skin is a major detoxification organ, and regular sweating, whether through exercise, infrared sauna, or hot baths, supports your body’s ability to clear hormones that would otherwise recirculate.
Infrared saunas are especially effective because they penetrate deeper into tissue than conventional heat and are well-tolerated even by people with fatigue or low tolerance for intense exercise. Aim for at least two to three sessions per week.
8. Reduce Stress and Prioritize Sleep
Chronic stress elevates cortisol, which directly suppresses progesterone production and worsens estrogen dominance. It also impairs thyroid conversion (T4 to T3) and raises reverse T3, compounding the thyroid-estrogen problem. Sleep deprivation has the same effect. Even a few nights of poor sleep can measurably lower progesterone and raise inflammatory markers.
Aim for at least 7 to 8 hours of sleep every night. Build in daily stress reduction through yoga, meditation, prayer, or whatever practice genuinely brings your nervous system down. This isn’t optional for hormonal recovery. It’s foundational.
9. Use Targeted Supplements to Support Hormone Balance
Several supplements have strong evidence for supporting estrogen metabolism and liver detoxification.
Diindolylmethane (DIM) or indole-3-carbinol (I3C) push estrogen down the protective 2-OH pathway.[2][3]
Calcium D-glucarate prevents reabsorption of estrogen in the gut by inhibiting the enzyme that deconjugates bound estrogens.[4]
Milk thistle supports liver phase II detoxification.
Fish oil and omega-3 fatty acids reduce inflammation.
Probiotics help maintain the gut microbiome, which plays a significant role in estrogen recycling through the enterohepatic circulation.
Also make sure you’re not deficient in magnesium, vitamin D, activated folate (methylfolate), B6, and B12, all of which are required for proper estrogen methylation and elimination.
MTHFR gene variants, which affect around 50% of people, can impair this step significantly.
10. Consider Bioidentical Progesterone Therapy
If you’ve addressed thyroid, diet, and lifestyle and still have estrogen dominance, bioidentical progesterone therapy can help directly restore the progesterone-to-estrogen ratio.
Unlike synthetic progestins, bioidentical progesterone matches the molecule your body naturally produces and doesn’t carry the same risks.
A typical starting dose is 20mg daily during the luteal phase, days 14 through 27 of your cycle, stopping if menstruation begins.
Work with a provider who understands bioidentical hormones and can monitor your levels appropriately. Progesterone works best as part of a comprehensive approach that also addresses the root causes above.
References
1. Krassas, G.E., et al. (1999). Disturbances of menstruation in hypothyroidism. Clinical Endocrinology. doi:10.1046/j.1365-2265.1999.00719.x.
2. Rajoria, S., et al. (2011). 3,3′-Diindolylmethane Modulates Estrogen Metabolism in Patients with Thyroid Proliferative Disease: A Pilot Study. Thyroid. doi:10.1089/thy.2010.0245.
3. Godinez-Martinez, E., et al. (2023). Effectiveness of 3,3′-Diindolylmethane Supplements on Favoring the Benign Estrogen Metabolism Pathway and Decreasing Body Fat in Premenopausal Women. Nutrition and Cancer. doi:10.1080/01635581.2022.2123535.
4. Calcium-D-glucarate. (2002). Alternative Medicine Review.
5. Krassas, G.E., Poppe, K., & Glinoer, D. (2010). Thyroid Function and Human Reproductive Health. Endocrine Reviews. doi:10.1210/er.2009-0041.






Thank you for sharing, Dr.Stanton.Glad that you mtenion that the first place the body stores fat is around the organs on our abdomen and initially remains not readily visible. Unfortunately lots of women don’t realize that even if they look skinny, they still need to watch what they eat and exercise at least two-three times a week, because they might be obese inside.Breathe, smile and be happy.
Hey Ruben,
Thanks for your comments!
What do you think about what Dr. David Brownstein says about heavy metals and hormonal system, specifically mercury:
“Dental amalgams (fillings) are the leading source of mercury toxicity….Mercury is a cell toxin that can disrupt the functioning of the entire hormonal system. The thyroid, hypothalamus, and pituitary glands are very sensitive to mercury.” (p. 187 of The Miracle of Natural Hormones by David Brownstein, MD)
I would agree with him, mercury disrupts the function of most tissues.
I was resently diagnosed with MTHFR A1298C homozygous gene defect. On top of that I hand and endometrium cyst on my ovary that was removed, however it turned out the stadium is so high that it spread over my other organs. Now I have a puzzle because I need to start the treatment for the gene defect meaning taking methylated vitamins and other supplements and make sure that my blood doesn’t clod. But also, I was told by the gynecologist that normally in this case he would prescribe his patient progesterone for half a year to remove all other endometriosis spots but in my case with the gene defect where the risk of clod is high he doesn’t recommend it. I was wondering if anyone has the same experience and actually decided to take progesterone with methylated vitamins, and if any what side effects occured?
Hey Ewelina,
You can look into supplements to help estrogen metabolism like DIM or indole-3-carbinol in addition to other lifestyle changes.
Your comment about TSH <2.0 doesn't mean you aren't hypothyroid…I think that's me! My TSH is always around 0.5. FT4 is around bottom 1/3 of the normal range. FT3 is at the bottom or below the normal range. TPO antibodies around 100. I self-diagnosed my Hashi's about 4 years ago…but the endocrinologist is just coming around now that I "might" have an autoimmune issue!! Otherwise, he says I have a form of untreatable hypothyroidism and says it is unlikely thyroid hormone replacement will help me feel any better. I think he won't treat me because my TSH is always low and doesn't follow the typical hypo pattern of high TSH, low free thyroid hormone levels. I asked him to check my pituitary as well to see if something upstream might be causing the low TSH, but hypo pattern, and he dismissed it. Any thoughts on why my TSH stays so low? Thx!
Hello, I am wondering if could clarify what you mean when you say, “You don’t have a estrogen problem if you have a thyroid problem!”
Hi Crystal,
What I mean is that low thyroid function can lead to the symptoms of excess estrogen, so if you have estrogen dominance or excessive estrogen then you first must rule out hypothyroidism as the cause. If hypothyroidism is the cause then treating this problem should result in improvement in estrogen levels.
Hello there. I have endometriosis and can really tell that every time my estrogen levels rise the inflammation in my gut/ovaries etc escalate. I get strong pains and very bloated. I started DiM/3IC recently and although it seems to help with some of my mood/estrogen dominance issues it seems to have caused a real flare in endo pan lasting two weeks now this has got me thinking – if the DIM ad a phytoestrogen will compete for the estrogen receptors What happens to the estrogen already there? Will the DiM cause an increase in estrogen ’floating around’ the before it Hopefully settles down? That could explain my flare maybe? I am not sure wether to continue or stop the DIM and am very frustrated. Really hope to hear from you.
Thanks for the information, l hope it’s going to help my daughter.