
What do hot flashes, fatigue, weight gain, and decreased sex drive all have in common?
They all may be the result of a condition known as menopause.
But these are not all of the symptoms associated with menopause.
Learn more about menopause symptoms including why they occur, which ones are most common, how to treat them and how to test to determine if you really are in menopause in this guide:
What is Menopause & What Causes it?
Menopause is a condition that ALL women will eventually have to deal with.
It is the result of ovarian failure to produce youthful levels of estrogen and progesterone (1).
Each woman has a finite amount of eggs that she is born with.
Each month (usually) an egg is “used up” during the ovulatory process.
Each month the total amount of eggs available declines.
Once the total amount of eggs reaches zero, she is unable to menstruate and menopause kicks in.
Menopause often results in rather dramatic symptoms which occur directly from the result of the withdrawal of estrogen and progesterone (2).
I referenced the word youthful in a previous sentence and that was by design.
Hormones, especially sex hormones, help manage very important processes in the body.
Processes such as the regulation of body weight, regulation of mood, regulation of sex drive, regulation of fertility, bone density, cardiac function, and so on.
The decline of these sex hormones in both men and women results in dramatic symptoms which can be attributed directly to the decline in hormones.
I keep mentioning the hormones because it is entirely possible to substitute or replace the lost hormones with a bio-identical version which can help manage the symptoms associated with this natural decline (3) (but more on that later).
Every year up to 1.5 MILLION women will transition from perimenopause into menopause.
That means that EVERY year 1.5 million women will have to deal with the symptoms associated with this condition.
This is no small number and it’s worth spending the time to talk about exactly what you will be experiencing.
Menopause will eventually occur as a result of time, pretty much no matter what.
But time is not the only cause of menopause either.
Surgical procedures, such as the removal of your ovaries (4), or certain medications, such as Arimidex (5), can completely shut off normal hormone patterns and result in what is known as premature menopause.
Regardless of how you reach it, the symptoms will often be the same.
So instead of focusing on the exact cause, it makes more sense to focus on the symptoms associated with the condition as well as the treatment.
With that in mind let’s jump into the symptoms…
The Most Common Symptoms of Menopause

It’s important to realize that each woman will present with slightly different symptoms when they enter menopause.
Some women may enter menopause and hardly have any difficulty with the transition while experiencing maybe some minor fatigue.
But why is this? Why is there so much discrepancy between individuals?
Much of this probably has to do with normal and innate differences in estrogen and progesterone levels.
Remember that the amount of estrogen (and progesterone) that you need to feel “optimal” is unique to your body.
This is why hormone replacement therapy cannot be standardized and requires a personalized approach.
It may be that some women experience only “small” drops of estrogen (those who have lower baseline levels of estrogen, to begin with) compared to some women who experience more dramatic swings in estrogen during menopause.
The more dramatic the drop in estrogen the more dramatic your symptoms.
Another reason that women may experience fewer menopausal symptoms has to do with baseline body fat and fat distribution.
Remember that the symptoms associated with menopause are caused by the abrupt withdrawal of estrogen from the ovaries.
But as your ovaries cease to produce estrogen, other areas of your body try to pick up the slack.
One area that attempts to do this is your fat cells.
Fat cells can turn testosterone into estrogen via a process known as aromatization (7).
The more fat cells you have the more estrogen you will produce.
Excess fat cells in the pre-menopausal woman may contribute to over-estrogen production (and estrogen dominance), but this same pathway may be protective against menopausal symptoms.
With all of these various factors at play, it isn’t difficult to see how some women may be hit harder by menopause when compared to others.
But how do these symptoms tend to present? How do you know you are in menopause?
The abrupt withdrawal of estrogen causes an array of changes that will affect the entire body (9).
Bones, brain tissue, fat cells, heart cells, and so on will all be affected by this change.
But some of these changes will be more noticeable than others.
In particular, there are 4 main areas that tend to be hit the hardest and are the most noticeable during menopause:
#1. Vasomotor Symptoms (hot flashes, night sweats, flushes, etc.)
Vasomotor symptoms are among the most common symptoms associated with menopause.
The term vasomotor is used to describe a series of symptoms such as hot flashes, night sweats, and flushes which all occur spontaneously and suddenly.
Believe it or not, the exact cause of these symptoms is not well understood!
These symptoms may be due to changes in cellular sensitivity to estrogen, changes in serotonin levels, or some other cause.
Hot flashes are present in up to 55% of women even before they experience menopause.
These vasomotor symptoms last an average of up to 5.2 years (10)!
They tend to occur spontaneously, may occur in the evening and or during sleep, and may occur several times per day.
During these episodes, your body will become flushed as blood flow increases to the surface of the skin.
These symptoms, because they are so uncomfortable, often lead patients to seek help.
The good news is that these symptoms can be completely controlled or eliminated with the use of hormone replacement therapy.
Providing the body with even small doses of estrogen (bio-identical) is enough to completely block these symptoms from popping up.
Even if you opt not to use hormone therapy for your vasomotor symptoms you should know that they will eventually fade over time.
But you may experience them off and on for up to 5.2 years before they stop completely.
#2. Vaginal changes (Vaginal dryness, pain with intercourse, and decreased libido)
Another important change that will occur during menopause is that of changes to the vaginal tissue.
The withdrawal of estrogen causes what is known as vaginal atrophy.
Estrogen naturally helps to keep the vaginal tissues healthy, moist and responsive to stimuli.
The withdrawal of estrogen causes them to atrophy (shrink) which may cause pain during intercourse, an increased risk of developing urinary tract infections, and cause vaginal pain.
Unlike vasomotor symptoms (which will resolve over time) these vaginal symptoms will NOT go away over time.
They are the direct result of reduced circulating estrogen in the body.
The good news is that you can “revive” vaginal tissues with the use of hormone replacement therapy (11).
Even if you don’t want to use systemic hormone therapy (such as a cream or gel) you can apply estrogen directly to your vagina to dramatically improve the tissues.
Topically placed estrogen (such as estrone) does not get absorbed into the entire system so the risk of negative systemic side effects is limited.
The use of topical estrogen is also sufficient to reduce the risk of recurrent urinary tract infections which can accompany vaginal atrophy.
It may be worth considering if you suffer from any of these vaginal side effects.
#3. Insomnia
Up to 50% of women who enter menopause report disturbance in the quality or duration of their sleep (12).
Sleep disturbances in menopause are probably caused by more than just one issue.
For instance:
It is well known that the quality of sleep tends to decline naturally with age (meaning the older you get the more likely you are to lose quality sleep).
But menopause adds another layer of complexity with hot flashes and night sweats.
It is not uncommon for women to wake up in the middle of the night (sometimes several times per night) due to changes in their body temperature or being drenched in sweat.
This is felt to be caused by hot flashes which occur during sleep and which are dramatic enough to wake the person up.
Unlike the other symptoms listed above, sleep may not necessarily improve with the use of hormone therapy.
If your sleep disturbance is due to hot flashes then estrogen therapy may help, but if it is due to a natural age-related decline in sleeping patterns, then hormone therapy will not help.
Managing your sleep is very important because sleep helps determine your mood and helps regulate your weight and sensitivity to other hormones.
#4. Mood changes
Women entering menopause are three times more likely to experience depression and anxiety (13).
Women already have an increased baseline risk of these conditions compared to men by a factor of two.
So when you combine menopause, this risk increases dramatically.
The exact cause of mood changes during menopause is not well understood, but it likely has to do with a combination of lack of sleep, estrogen changes, changes in body weight, changes in other hormone levels, and so on.
As an example:
Menopause may lead to hot flashes which lead to insomnia (lack of sleep), which leads to daytime fatigue, which then leads to issues at work or with relationships which then may lead to depression.
Depression, like insomnia, may not necessarily resolve with hormone replacement therapy.
Other Symptoms
The big 4 symptoms listed above are not the only symptoms of menopause.
In fact, estrogen withdrawal will affect other tissues in your body as well.
I’ve included a list of other symptoms which you may experience as you transition into menopause below:
- Weight gain (14) – Women gain up to 15 pounds on average during menopause.
- Hot flashes
- Reduced “glow” of the skin – Estrogen helps provide the “glow” to the skin that women experience (especially during pregnancy).
- Loss of subcutaneous fat (15) – Loss of subcutaneous fat deposits in the face and hands lead to “shrinking” of the skin. Topical estrogen can restore this fat and bring back a more youthful appearance.
- Increased skin wrinkling (16) – Estrogen is considered a youthful hormone and as it declines you will notice more wrinkles and age spots.
- Fatigue
- Decreased libido (17) – Vaginal dryness and pain during intercourse may reduce your libido or sex drive.
- Insomnia
- Joint pain
- Depression and/or anxiety (18)
- Bone loss (19) – Estrogen and progesterone help maintain bone strength and density, as estrogen declines during menopause you will be at increased risk of developing osteopenia and osteoporosis
- Increased risk of heart disease (20)
- Poor concentration
- Poor memory
- Increased risk of Dementia
- Hair loss or hair thinning
- Increased risk of developing urinary tract infections (21)
- Increased risk of developing incontinence
- Bloating or fluid retention
- Acne
Testing for Menopause
What if you are experiencing the symptoms but are not sure if you are in menopause?
Can you test for menopause using standard blood tests?
The answer is yes (22).
Most physicians don’t routinely test for menopause because they generally don’t treat it with bio-identical hormones, but there is definitely an easy way to test for menopause.
This may sound strange to you at first but it’s definitely the truth.
If you don’t plan on treating a condition then why do you care if someone has that condition?
It’s helpful for the patient to know and understand what is happening in their own body, but from the perspective of the physician, it’s not always felt to be important.
I strongly believe that you should be aware of your body and it’s very helpful to know if you are in menopause or not, which is why I’m discussing this post and how to test for it.
So how do you do it?
The best way to do this is by ordering a couple of standard hormones.
The following labs can be used to test if you are in menopause:
- FSH (follicle-stimulating hormone) – Perhaps the best way to diagnose menopause is to order the FSH test which stands for follicle-stimulating hormone. A high FSH, in the presence of menopausal symptoms, is usually sufficient to diagnose menopause. An FSH greater than 22.3 IU/l may be indicative of menopause (23).
- Estradiol – During menopause estrogen levels fall. The most potent and powerful estrogen in the body is estradiol (though there are others) and this value will DROP during menopause. Estrogen levels vary dramatically between individuals but look for a VERY low estrogen level as an indicator that you are in menopause.
- Progesterone – Progesterone, much like estrogen, will DECREASE during menopause. Look for a VERY low progesterone level as an indicator that you are in menopause.
See examples of labs that indicate progesterone below:
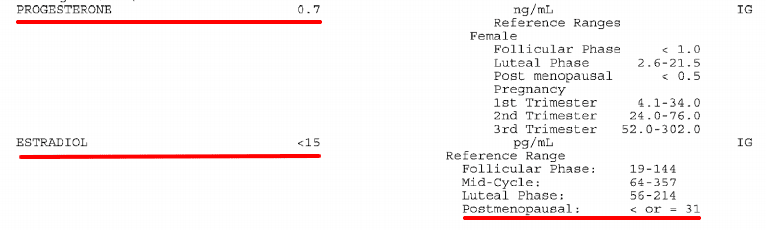
You can see in this example that the progesterone is 0.7 ng/mL which is less than 1.0 and VERY low.
The estradiol is so low that it cannot be measured and is referenced as being less than 15 pg/mL.
Women in menopause will often present with labs VERY similar to these.
In menopause several things happen:
#1. Your body stops ovulating and estrogen levels fall.
#2. This drop in estrogen causes FSH to rise (as your body tries to kick estrogen back into gear).
#3. Your ovaries don’t respond to FSH so estrogen levels and progesterone levels stay low while FSH levels stay high.
#4. FSH, estrogen, and progesterone can then be used to help diagnose what is happening in the body.
This series of events is helpful, but only if you are NOT currently taking hormone therapy!
Oral contraceptives (birth control pills) or bio-identical hormones will make these tests less helpful.
So only ask for these tests if you are NOT taking any hormones.
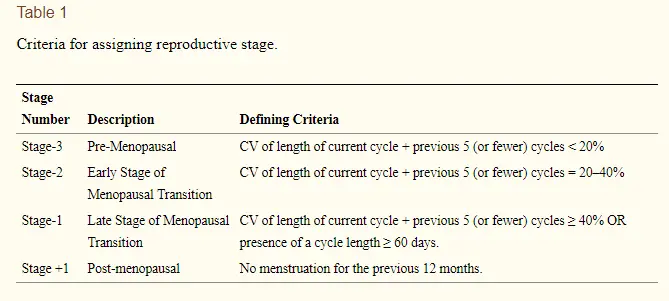
Perimenopause vs Menopause
What about perimenopause?
Perimenopause is considered to be the state which occurs PRIOR to menopause (24).
You can think about perimenopause as a condition that develops as your body progresses from menstruating to menopause.
Perimenopause is often associated with many symptoms, but these symptoms are not quite as intense when compared to the symptoms of menopause.
In perimenopause, the body is still producing SOME estrogen, but this estrogen is much less than what would be considered normal for the body.
During this period you may experience irregular periods, increased episodes of menstrual bleeding, and even minor symptoms of menopause off and on.
Remember:
Menopause kicks in when estrogen drops to near zero.
In perimenopause, your body is still producing SOME estrogen but it’s very sporadic and may occur in small doses or large doses off and on for many months.
Perimenopause can be differentiated from menopause in how it presents, how long it lasts, and the severity of symptoms.
Estrogen and progesterone levels will often be sporadic and inconsistently high and then low.
FSH will often be borderline high, but not quite in the menopausal range (as indicated above).
Symptoms of menopause may come and go in between menstrual cycles and as estrogen fluctuates.
As long as you are still having menstrual cycles you are NOT in menopause.
Perimenopause can be treated with smaller doses of hormones much like menopause.
Final Thoughts
Menopause is a state which all women will eventually experience.
This condition occurs as the female body ceases to ovulate and ceases to produce healthy and normal levels of estrogen and progesterone.
The symptoms associated with menopause can vary from mild to severe and potentially life-altering.
Estrogen has a powerful and potent influence on many cells in the body ranging from fat cells to brain cells to heart cells and so on.
Because of this wide-ranging action, you may experience symptoms such as fatigue, hot flashes, bone loss, depression, and weight gain during menopause.
Menopause can be treated with bio-identical hormone replacement therapy (meaning the use of natural hormones) which can completely eliminate and stop these symptoms.
Perimenopause is the condition that occurs immediately BEFORE menopause and it is often associated with minor menopausal symptoms which fluctuate for 6 to 12 months.
Testing for menopause can be accomplished by ordering FSH, progesterone, and estradiol levels.
Now I want to hear from you!
Are you suffering from the symptoms of menopause?
Are you currently getting treated?
Did treatment help reduce your symptoms?
Have you used natural therapies? Have they worked?
Leave your comments below!







Hi Dr. Childs
I would like to know if there might be any connection between experiencing Perimenopause symptoms for over 8 years now (no treatment was offered), and being recently diagnosed with Hashimoto’s thyroiditis?
Thank you in advance.
Hi Nicoleta,
Thyroid disease can cause issues with progesterone:estrogen levels which may lead to some of the symptoms you are experiencing. It’s hard to say without more information and testing, though.
Thank you, Dr. Childs, for all you do to inform and educate. I started learning here awhile back for my thyroid …and now am returning to learn about all things Menopause. I feel like I’ve read (and understood!) nearly every article you’ve written on these topics.
You are a Godsend to clearly explain your topics and to reference sources. IT IS MUCH APPRECIATED~ keep up the good work! The world needs experts like you who are willing to share your expertise and knowledge for those of seeking healthy living!
Hi Jana,
You’re welcome! And I’m glad you found it helpful.
I find this comment to be suspect, “Once the total amount of eggs reaches zero, she is unable to menstruate and menopause kicks in.”
No Gyn has ever said that to me, nor have I ever read that in any publication before. I also know that three years post-menopause not only DID I have follicles leftover, but for reasons unknown to either the doctor or myself, they were developing, I was bleeding, and biopsies proved zero malignancies. I believe you are mistaken on this.
Hi Pamela,
What I’ve stated here is considered to be common knowledge. Like anything in medicine, however, there are always exceptions and people who don’t fit the standard mold but this is considered to be the prevailing thought on what probably triggers menopause. Here is the source straight out of an endocrinology textbook:
“Every month a new egg matures inside a follicle in an ovary. The follicle produces hormones itself. If the mature egg is not fertilized after it is released from the ovary (ovulation), the woman has a menstrual period. During the time leading up to menopause the ovaries gradually make less and less hormones. A woman has reached menopause when her ovaries stop releasing eggs.
It is thought that all of the egg cells a woman will ever have are already inside her ovaries when she is born. There is probably a link between the time when a woman reaches menopause and the time when her supply of egg cells is used up. Before the age of about 40, the number of follicles that mature decreases gradually. After that, the number decreases quite quickly, until no more follicles mature.”
Link: https://www.ncbi.nlm.nih.gov/books/NBK279311/
As an aside, if you are relying upon your gyn to give you hormone recommendations and information then you will find your information will most likely be woefully inadequate. Again, the information I’ve cited above is textbook medicine so if they haven’t offered it to you it’s probably because they forgot or aren’t aware of it.
My original statement could probably be made more accurate by re-stating it to say something similar to “for most women, menopause is triggered as her eggs are depleted”.
During Perimenopause I used:
1. Black Cohash 120mg to 160mg BID
2. Calcium 1000mg/Magnesium 400mg/Zinc 15mg +D3 600IU BID (amounts based on 3 pill total)
3. Fish 800mg /Flax 800mg/Borage Oil w/Evening Primrose & Black Current Oils 400mg BID (amounts based on 2 pill total)
4. Ester C 1000mg BID
5. K2
6. B6
7. Biotin
8. Glucosamine/Chondroitin/MSM plus Hyluronic Acid
I tried a few other supplements, but I found that these above made the most difference. Calcium was HUGE in maintaining a sense of calm. One week I ran out of my Calcium/Magnesium/Zinc +D3 and had to resort to a bottle of Calcium tablets my DMiL had left for me a few months ago. By the end of the week I was tearing the heads off of my entire family when I happened to look up to see their faces; I felt horrified with myself. I went to the store and bought a bottle of my Calcium/Magnesium/Zinc +D3 and started on it right away, not caring that I had just overdrafted my account to do so.
For many years this combination of supplements eliminated Night Sweats and Hot Flashes, but towards the end I had breakthroughs of each. Always the Night Sweats came first. At almost exactly 1 year post menopausal my Hot Flashes became Blast Furnace HOT FLASHES. I would turn red and sweat would pour down my face, neck, back, and chest. I was very grateful to have been retired, I would put down whatever I was doing and just strip off my clothes. After 4 months like this I made an appointment and asked for something I never ever thought I would, HRT. Prempro worked fantastically and I used it for five years where upon I gave it up on my own by titrating it down slowly. I didn’t die. For about a year I wanted to. Eventually though most of the hot flashes ended, occasionally I get one on hot summer nights.
Hi Pamela,
Thanks for sharing what worked for you! Your list corresponds closely with what I typically recommend which can be found here: https://www.restartmed.com/estrogen-supplements/
Hi Dr. Childs!
If this statement is true:
“Menopause can be treated with bio-identical hormone replacement therapy (meaning the use of natural hormones) which can completely eliminate and stop these symptoms. ”
Then WHY isn’t this the FIRST thing prescribed for women going through menopause?!
If Bio-Identicals HRT “completely ELIMINATES and STOPS” these symptoms…why aren’t they the first thing that the Doctors go to and prescribe?!
Millions of us Women are SUFFERING through these HORRIBLE symptoms…millions of Women have had to juggle everyday life along with these horrible symptoms…
WHY wouldn’t these Doctors want INSTANT RELIEF for their patients so that they can ENJOY QUALITY OF LIFE?!
“Most physicians don’t routinely test for menopause because they generally don’t treat with bio-identical hormones, but there is definitely an easy way to test for menopause.”
WHY?!
I guess you answered my WHY with:
“If you don’t plan on treating a condition then why do you care if someone has that condition? ”
This mindset in today’s world is completely unacceptable!!! We women endlessly contribute to the good of our society and DESERVE to live a quality life!
I’ve read many comments from women on BIO-Identicals who said they are a Godsend! That they made them feel “normal again” and completely got rid of the horrible symptoms of menopause!
It’s ridiculous to keep chalking up menopause as a “normal thing that women just need to deal with”
We are sooo advanced with technology…we Women shouldn’t have to continue “dealing with these symptoms with NO reprieve”…we Women shouldn’t have to keep experimenting with supplements that MAY or may NOT work to alleviate these horrible symptoms…WHEN there is an INSTANT cure!
Why have millions of women had to suffer when there is an INSTANT solution?!
Thank You For Reading My Passionate Rant!
KC Plummer
Hi KC,
I would say that bio-identical hormones could instantly resolve menopausal symptoms in 8 out of 10 women and it will take a little longer in the last 20 percent but it’s still possible.
The why doctors aren’t aware is actually quite simple. They are really never taught about hormones and they believe that all hormones increase the risk of breast cancer and stroke based on some old studies in non-bio-identical based hormones. More concerning is that recently there has been a push (by pharmaceutical companies) to completely ban these medications because they say they are dangerous.
It’s a crazy world we live in when some of the best therapies available to men (testosterone) and women (bio-identical hormones) are at risk of being taken away.
Hi,
I’m 52 and have been experiencing menopause symptoms (primarily hot flashes/night sweats) on and off for the last 3 years. I still get an irregular period every 4 -6 months, so not quite menopause yet. When the hot flashes got worse for a couple of months last year, my doctor (an “integrative” family doctor) prescribed the estrogen patch at .025 mg. No hormone testing was done. The patch works great – hot flashes disappeared after a week on the patch (and it’s now been 8 months) and other less noticeable issues improved (dryness).
My problem is with the progesterone (oral, bio-identical): at first, I tried 10 days a month on 200 mg., then every day on 100 mg. Either way, I feel awful when I take the progesterone, it seems to affect my mood. My doctor is not receptive to using progesterone cream or to decreasing the dosage, she’s stuck on some set (uniform) protocol concerned with endometrial cancer, even though I’m using a low estrogen dosage and react badly to the oral progesterone. BTW I don’t have heavy periods or any breakthrough bleeding. Any thoughts?
Hello Dr. Childs,
My daughter has been diagnosed with Premature Ovarian Insufficiency at age 16, based on her high FST, LH and almost non-existent estradiol and progesterone. Her menstruation suddenly stopped when she was 15 (while being regular the previous 3 years). A few months prior to her menstruation abruptly stopping she had a bout of Mono. After the POI diagnosis, we also accidentally found that she has a thyroid nodule. We’ve done extensive blood work to rule out genetic diseases and autoimmune diseases related to the POI but we found none. We do not have anyone in the family with such a problem. I keep thinking there must be a connection between the POI and her thyroid issues, but no one has been willing to even venture a hypothesis. I just can’t figure out what might have caused all these serious problems for my daughter who I’ve raised with organic, homemade food, always cautious about environmental factors and toxins, etc. I know that there is very little research about POI, and especially in girls as young as she is, but I wanted to see if you’ve read something on the matter, and if you think there might be a possible correlation between her thyroid and POI. ( I should mention that her thyroid panel is not optimal – TSH between 1-2, RT3 – 23, Free T3 – 3.7, Total T3 – 127, TPO AB – 9, and her thyroid nodule is 1.5cm x 1m, enough to necessitate two biopsies, both of which came back ambiguous)
Thanks a lot for your time and help!
Hello. I was officially diagnosed as right in menopause back in December 2021. My symptoms have been extreme fatigue, sleeping a lot during the day (to where my husband thinks I’m either on drugs or just lazy), painful intercourse, increase in UTI’S, annoyed easily. It certainly affects my everyday life with depression and anxiety as well and I tend to prefer to stay home than go anywhere and interact with others. I have zero energy with two teen boys and an 11 year old son with Autism and I feel like I’m failing them in every way. And let’s not forget the constant sweating and hot flashes, those are fun. I’ve been told by some acquaintances their symptoms lasted 10 years…TEN YEARS! Is this how long I could possibly have to look forward to the gift that keeps on giving? Its affecting my daily life, my mood, my brain, my memory, my health/weight (80lbs overweight now) and my marriage.
Hi Lisa,
It seems to impact some women more than others but, typically, most women don’t have to deal with it for that length of time, at least not at full force. There are treatment options, though, including the use of bioidentical hormones (HRT) which can completely eliminate symptoms in most cases. If it’s severely impacting your quality of life then looking into treatment is probably a good idea: https://www.restartmed.com/biest/
I had a Surgical Menopause @ age 44 for extensive, long standing Endometriosis since a teen. Violent daily pelvic pain, endometriomas, & yrs of Progestins to suppress endo, several laparoscopies. I kept one ovary at hysterectomy that never functioned post op. Menopause was severe & immediate. I was a very physically fit, thin, healthy energy female at time of surgery. The Endometriosis surgery didn’t provide pain relief, had surgery at Yale 23 years ago. Never able to take ANY HRT after surgery as it made endometriosis pain intolerable. Menopause was severe.
I’m now 67, no libido or sex too many yrs to recall, constant pain from Burning Mouth Syndrome x 8 yrs (Glossodynia), poor sleep, little energy, depression.
In my late 30’s Endocrinologist put me on Synthroid for severe Hypothyroidism. Endocrinologist told me I had Hashimoto’s, (long family hx of thyroid abnormalities on maternal side) plus severe B12 deficiency. Been on B12 Hydroxy injections since my 30’s. Synthroid was discontinued by Endocrinologist after 2 years as he followed my labs & continued to monitor my thyroid annually.
I have no quality of life & am no longer the vibrant person I Always have been. Have Gained 25 lbs (140 lbs. currently) in last 5 years. I have tried hard to lose weight to no avail.
Fat is in abdomen & breast. I am PETITE 5’5”. Hormones send endometriosis soaring. I have early osteoporosis. I hate how I look now, the constant oral neuropathic pain (LSU OROFACIAL SPECIALIST diagnosed).
My Thyroid labs this summer (2022), show my TSH 1.176 (0.400-4.000 ulU/mL normal range).
This Endocrinologist told me all my lab results were normal. I was thinking maybe the bizarre weight gain, lack of energy, depressed mood might be related to thyroid or Endocrine system. I barely eat any food. If I do, my weight is up by next day. Is this TSH 1.176 indicative of suboptimal function?
Hi Elizabeth,
Not necessarily, but you would need additional thyroid tests to accurately make that assessment. Please see this article which discusses which additional tests you would need as well as the optimal ranges for each: https://www.restartmed.com/normal-thyroid-levels/